


Abstract
The marked increase in deaths related to opioid drugs after 1999 was associated with an increase in the number of prescriptions for opioid drugs. This was accompanied by increasing demand for improved management of chronically painful conditions. These factors suggest that improvements are needed in the education of physicians with regard to the management of chronic pain, the optimal therapeutic application of opioid drugs, and the avoidance of substance use disorders. In this article, we address the evidence that physician education can influence prescribing practices and we discuss approaches to enhance the preclinical and clinical education of medical students in pain management and substance use disorders.
Introduction
Deaths related to opioid1 drug overdoses have been rising in the United States since 1999 and they continued to rise at an increasing rate through 2017. Deaths attributable to overdoses of synthetic opioids other than methadone increased on average 71% a year from 2013 to 2017 (Hedegaard et al., 2018). A significant factor in the increase in opioid-related overdose deaths after 1999 was a marked increase in the number of prescriptions for opioids, often for nonterminal pain-related conditions. However, by 2011 (Warner et al., 2011), concerns that opioid drugs were being overprescribed for some patients and by some health care providers resulted in pressure on prescribers to reduce the number of prescriptions; by 2013, the rate of opioid prescribing had stabilized (Dart et al., 2015). Nevertheless, despite the leveling off in the prescription rate, opioid deaths continued to rise as some patients unable to obtain prescribed opioids turned to illegal sources for their opioid supply. At the same time, the availability of the very potent opioid drug fentanyl increased considerably, and this agent was often used to “cut” batches of illicit heroin (Rothberg and Stith, 2018) to an extent that varied considerably from batch to batch. Batches of heroin containing significant amounts of fentanyl greatly increased the risk of respiratory depression and death, contributing significantly to the progressive rise in overdose rates. There is experimental evidence in rats showing that the addition of fentanyl to heroin substantially prolongs the duration of brain hypoxia relative to either drug given alone (Solis et al., 2017).
Given the many complex factors underlying the continuing upward trend in opioid-related deaths, it is obvious that a multifaceted approach is needed to address this major public health crisis. We now have greater insight into the complex interrelationship between the varying pharmacologic properties of different opioid drugs, the constantly varying accessibility of different opioids from both legal and illegal sources, and the high potential for unanticipated negative outcomes when legal and health policy initiatives are undertaken without careful evaluation of potential unintended consequences. All of these factors point to the need for improved education of prescribers as one key factor in counteracting what has become known as the opioid crisis. Physicians need to be better prepared than in the past to manage patients with nonterminal pain conditions who need effective pain control while reducing the use of opioids whenever possible.
There is evidence that the education received by a physician has a significant influence on the physician’s later opioid prescribing patterns. The rates of opioid prescribing vary markedly between individual physicians. Schnell and Currie (2018) demonstrated that there is an inverse relationship between the number of opioid drug prescriptions written by a physician and the rank of the medical school where the physician trained. This inverse relationship was particularly strong for primary care providers, the specialty responsible for the largest number of opioid prescriptions, and was weaker in specialties where there is a requirement for postgraduate training in the use of opioids (e.g., pain medicine, anesthesiology). There is also evidence that patients receiving prescriptions for opioid drugs from physicians who exhibit high rates of prescribing opioids during emergency room visits are more likely to be “long-term” opioid users, receiving prescriptions for opioids for 6 or more of the 12 months after the emergency room visit, than patients treated by physicians with low rates of opioid prescribing (Barnett et al., 2017). Thus, early education of physicians in optimal practices for the prescription of opioids is associated with reduced patient vulnerability for the subsequent development of substance use disorders and can be expected to foster healthy treatment approaches that will last throughout the physicians’ careers.
Until recently, substance use disorders were not covered extensively in the 4 years of undergraduate medical education. The pharmacology of addictive drugs was described in the preclinical pharmacology course, with varied additional coverage in clinical clerkships. As the magnitude of the overdose crisis became apparent (around 2010 to 2011), more attention has been paid to ensuring that physicians in training receive a more comprehensive overview of the complex problems underlying the misuse of prescribed opioid drugs. At Uniformed Services University (USU), a decision was made to replace a discipline-based preclinical curriculum with an “integrated” curriculum, for reasons that were unrelated to the opioid crisis; the “new” curriculum was implemented in 2011. In meeting the emerging educational goals of the medical school in many areas, this programmatic change in the organization of medical education also presented an opportunity to develop a more interdisciplinary approach to instruction in the areas of pain management and substance use disorders, with particular emphasis on the opioid crisis, since the magnitude of this health care disaster was beginning to be recognized at roughly the same time. As part of the overall curriculum reform process, teams of faculty were assigned to review and refine the curriculum in discrete topic areas.
With regard to substance use disorders, there was general agreement on several general principles that should underlie the revised curriculum; these general concepts are summarized in Box 1 and discussed further in the following sections. Although this was not an initial feature of our revised curriculum, by 2015 there was also agreement that the terminology related to the use of potentially addicting drugs should be modified in all teaching materials and presentations to be consistent with the recently released fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) terminology (e.g., “opioid use disorder” not “opioid addiction,” and so forth; Hasin et al., 2013). All teaching materials have been updated to be consistent with DSM-5. We regarded this as an important change, since there has been concern for some time that a few physicians and health care providers have unrecognized biases against persons with substance use disorders. Terminology employing words and phrases that might be considered judgmental in thiscontext can itself perpetuate the bias, with negative effects on the quality of health care provided to these patients (Corrigan and Nieweglowski, 2018).

Basic Principles
Integrating Education across Disciplines in the Undergraduate Medical Curriculum.
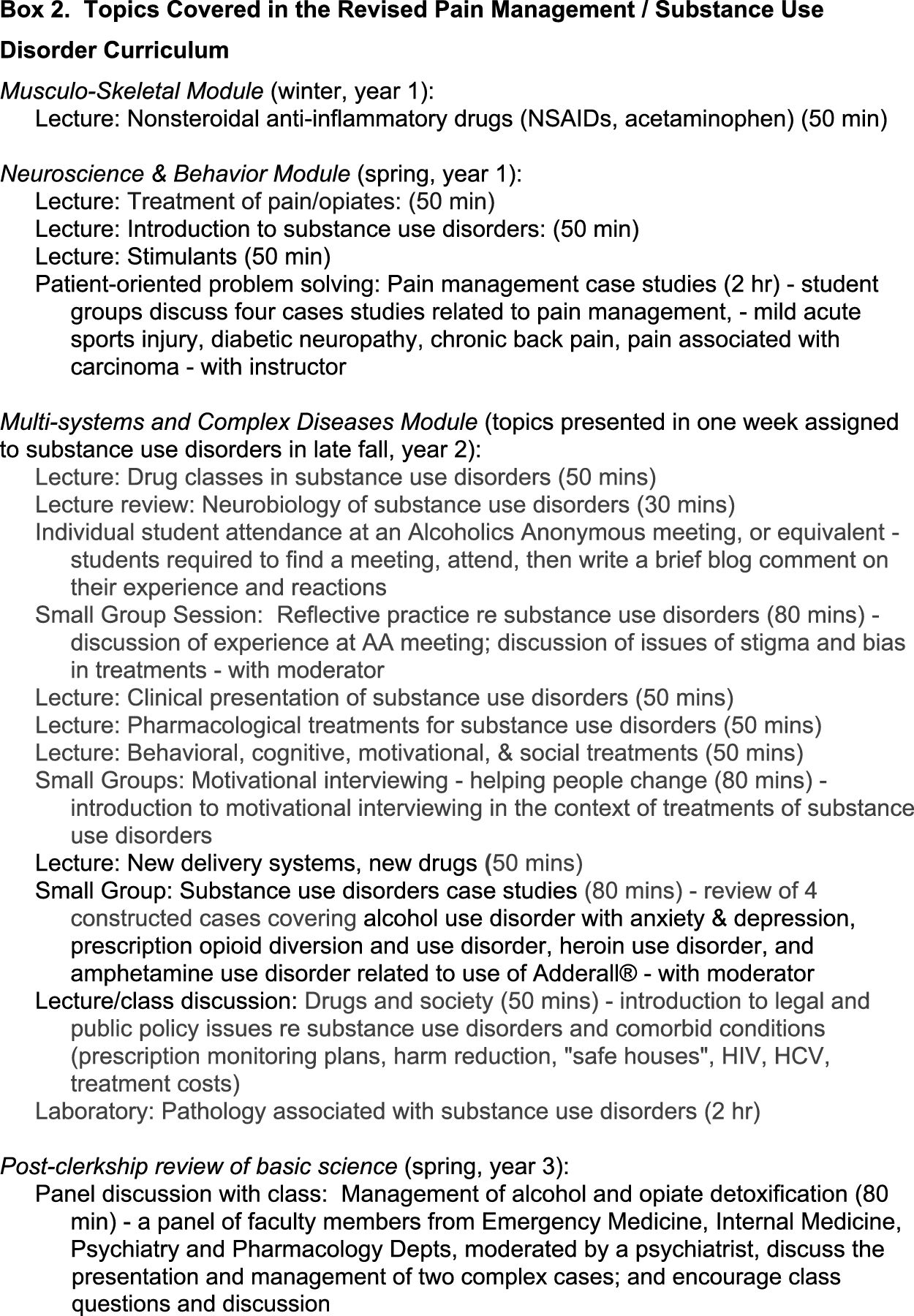
An initial goal of the new curriculum was to increase integration of instruction relating to substance use disorders across the relevant disciplines in the preclinical and clinical curricula. Prior to the introduction of the new curriculum, faculty from the departments of pharmacology, medical and clinical psychology, and psychiatry met to develop a coherent sequence of classes that progressed from drug use and alternative therapies in the management of mildly painful injuries to the management of severe pain, to the inappropriate use of prescribed opioids and the risks of development of opioid drug use disorders. Discussion of pathology associated with substance use disorders and drug overdoses was also programmed within this set of classes. Over time, and as faculty from each department became more familiar with the content deemed critical by each department to meet the needs of U.S. Medical Licensing Examinations (USMLEs), the sequence of lectures was revised with more coordinated content to provide a more coherent approach to substance use disorders (Box 2).
Relating Discussion of Opioid Use Disorders to the Management of Chronic Pain Conditions.
The increase in opioid-related deaths since 1999 occurred predominantly in an older age range of subjects than the predominant age range for heroin-related deaths in the decades prior to the onset of the opioid crisis (Warner et al., 2009). The data also showed that prescribed opioids, not illicit opioids such as heroin, were the major drug class contributing to the increased number of overdose deaths in this older age group (Warner et al., 2009, 2011). We therefore decided that the opioid drug crisis must be presented in the context of the management of chronic nonterminal pain conditions. The mortality data, drawing attention to the substantial involvement of prescription opioids in the increased death rate, suggested that poor management of prolonged nonterminal pain conditions was a significant contributing factor. In developing enhanced consideration of the optimal clinical use of opioids in pain management, we relied heavily on current clinical practice guidelines, including the 2016 U.S. Centers for Disease Control and Prevention (CDC) guidelines (Dowell et al., 2016) for prescribing opioids for chronic pain. We also ensured that the material was consistent with the Joint Pain Education Program developed by the Defense and Veterans Center for Integrative Pain Management, which places emphasis on nonpharmacologic methods, including local heating or cooling (depending on pain location and type), acupuncture, transcutaneous electrical nerve stimulation, and the use of acetaminophen or nonsteroidal anti-inflammatory agents for the treatment of acute or chronic pain, with an emphasis on minimizing the use of opioids in pain management. Evidence of efficacy of some nonpharmacologic pain therapies is limited, but recent meta-analysis reviews of exercise and acupuncture offer support for their clinical efficacy in some painful conditions (Goh et al., 2018; Armour et al., 2019), and acupuncture and transcutaneous electrical nerve stimulation are now widely available in pain clinics and in the Military Health System.
It should be noted that clinical practice guidelines are very helpful in guiding therapies but can have unintended consequences if the guidelines are applied in an inflexible way or imposed in situations that are outside the domains for which the guidelines were developed. This appears to be a particular problem with respect to the 2016 CDC guidelines on the treatment of chronic pain (Dowell et al., 2016), in which some patients already receiving opioids in dose levels above those recommended in the CDC guidelines (for the initiation of new opioid treatment regimens) have suffered an abrupt reduction or discontinuation of prescribed opioid doses, sometimes leading to withdrawal.
Integrating Discussion of Opioid Use Disorders with Other Substance Use Disorders.
Although the inappropriate use of prescribed opioids became a major emphasis in the revised curriculum, there was consensus that it was important to consider the basic features of opioid drug toxicity, dependence, and withdrawal in the context of other substance use disorders. Time was created in the Multisystems and Complex Diseases module constituting the last segment of the preclinical curriculum for a week of instruction on substance use disorders, including alcohol use disorder and its treatment (because of the significant incidence of this disorder in the populations receiving medical care from our graduates who will serve military personnel and their dependents; Schumm and Chard, 2012). The module also covered stimulants and hallucinogenic agents, in addition to opioids, permitting us to note similarities and differences in targets, mechanisms of action, and available therapies for each drug class. Consideration of nicotine and tobacco use presents a challenge with respect to the optimum location in the curriculum. The basic pharmacology of nicotine is best discussed along with other drugs acting primarily on the autonomic nervous system; in our curriculum, these are covered in the Cardiovascular, Pulmonary, and Renal module. However, the central actions of nicotine on reward pathways (de Kloet et al., 2015) need to be considered in the context of other substance use disorders; parallels between nicotine, opioid, and alcohol effects on dopamine pathways help reinforce understanding of the actions of each of these drugs. We also discussed novel drug delivery systems (e-cigarettes and vaping devices such as Juul), presenting an opportunity to emphasize the general significance of the route of administration in establishing patterns of drug self-administration (Hines et al., 2017). Time was also assigned to coverage of newer recreational drugs including synthetic cannabinoids and cathinones.
Creating a Thread Connecting Substance Use Disorder Instruction across 4 Years of the Curriculum.
Understanding and retention of relevant information was facilitated by repeated exposures to related materials, presented in a sequence of increasing complexity. The recent increase in opioid overdoses is at least partially related to their inappropriate use in the treatment of chronic severe nonterminal pain syndromes (Warner et al., 2011; Barnett et al., 2017), and this topic is now discussed at multiple places in the medical curriculum in the context of pain management in general. Initial discussion focused on the management of mild sports-related injuries, in which the relatively transient and mild nature of the pain clearly does not warrant the use of opioid drugs. Subsequent discussion evolved to the treatment of pain in patients with terminal cancer for which opioids are often the only effective approach to pain management. After these extremes were discussed, the place of opioids in the treatment of severe nonterminal pain conditions, where opioids may provide some relief but frequently do not provide effective continuous relief over months or years and often lead to inappropriate use and the development of dependence on the drug (Murray et al., 2019), could then be given appropriate emphasis. A list of the topics covered in the revised curriculum is contained in Box 2.
To implement this objective, we constructed a small number of “cases” in which a fictional subject is followed as his or her disorder progresses from initial presentation to effective treatment or the development of a use disorder. Some of these “cases” thus appear in small group discussions in multiple modules in the preclinical curriculum. In developing “cases” related to substance use disorders, we focused on topics of relevance to military physicians, including alcohol misuse, prescription opioids for painful nonterminal conditions associated with battlefield injuries, and inappropriate use of stimulants. Box 3 describes the history of “George,” who progresses from a mild work-related back injury to opioid use disorder and eventually to opioid withdrawal. George’s problems are covered in small group discussions in three different modules within the 18-month preclinical curriculum. (The full case notes provided to students contain more clinical description than the brief summary presented in this article.)

At this point in the evolution of the USU curriculum, education on substance use disorders in the clinical years of the medical curriculum had received less focused attention than in the preclinical curriculum. In part, cases considered during clinical clerkships depend on the patients presenting during the clerkship. Moreover, the “no tolerance” policy of the military services toward the recreational use of psychoactive drugs in military personnel means that our students usually see few if any such patients experiencing acute intoxication and/or withdrawal during this period. Clinical practice guidelines for the treatment of chronic pain conditions in military personnel, their dependents, and retirees (e.g., https://www.dvcipm.org/clinical-resources/joint-pain-education-project-jpep/) now focus on avoiding prescription of opioids when alternatives are available, and nonpharmacologic approaches to pain relief are now favored whenever possible and appropriate. The USU Department of Psychiatry has also introduced a multidisciplinary panel discussion for third-year students on the management of alcohol and opioid withdrawal. This class, presented after students have completed a year of clerkships, utilizes a panel consisting of an emergency room physician, an internist, a psychiatrist, and a pharmacologist to discuss the underlying principles and the optimal approaches for the treatment of a patient with a heavy alcohol habit who presents with numerous problems as he enters withdrawal and for withdrawal in a patient who initially received prescription opioids for a pain condition but progressed to an opioid use disorder. These case descriptions contain more clinical detail than in the second-year cases. Students are asked to suggest the optimal management of issues that arise for patients as withdrawal progresses and treatment is implemented, and panel members comment on the responses, discuss the background to each issue, and note the unique concerns of specialties in relation to this case.
Consideration of cases in the small group classes in year 2 of the curriculum and the panel discussion in year 3 provide an opportunity for instructors to initiate discussion of the complexities and ethical/moral concerns regarding prescribing opioids to patients, given the propensity of these drugs to lead at a later time to opioid use disorder. Instructors point to the challenges for the physician in considering whether an opioid prescription that appears to be required for adequate pain relief but may result later in opioid use disorder is appropriate, while at the same time avoiding bias against specific categories of patients.
Expanding the Use of Small Group Instruction.
Substance use disorders have a complicated etiology and a complex and varied presentation. There may also be strongly conflicting views among students on these disorders and appropriate treatment options. It is therefore important to allow students ample time to discuss their views in a neutral but moderated environment. Well managed small group sessions provide an excellent way to meet this goal (McClurg et al., 2015). In our experience, student groups often contain members who are very well informed on the topics and others who have little information beyond what they have gathered from the popular press and media. Small groups also allow time for discussion and the review of complex concepts that are well represented in the national board examinations, covering issues as varied as the molecular and anatomic targets for drugs implicated in substance use disorders and the critical relevance of availability of drugs via inappropriate prescribing or from community sources. The varying characteristics of each predictable stage of the condition (i.e., intoxication and regular use, withdrawal, detoxified but in danger of relapse) strategically guide selection of the most appropriate treatments. Moreover, the expression of these phases differs critically during and after chronic exposure to different drug classes. Students are assigned to groups of about 8–12 students lead by a faculty mediator; group assignments are different for each class. Most small group discussions are focused around a PowerPoint presentation based on cartoons and animations depicting background information or case descriptions, followed by questions for class discussion. These presentations guide the session and help to ensure that all groups cover the same content. Prior to each session with the students, all small group instructors (including faculty) review the presentation materials together to familiarize themselves with the material, to update or revise the presentation where needed, and to learn from collective experiences and knowledge related to the subject. This helps to ensure consistency in coverage across 12–18 small groups conducted simultaneously. In addition to reviewing the fundamental science underlying the actions of the drugs, instructors are encouraged to direct discussion to cover other relevant issues such as the reliability of self-reported pain in patients who might be prescribed opioids and when and how to evaluate whether opioid use disorder might be present. The group setting also provides an opportunity to address issues related to physician bias and the racial disparities that have been reported in the management of chronic pain and the prescription of opioids (Burgess et al., 2014; Gaither et al., 2018).
Understanding Social Context.
The inappropriate use of psychoactive drugs is highly sensitive to drug availability and the social context in which the drugs are used. Legislation imposing criminal penalties on the sale and possession of some drugs while permitting the legal use of others has had a major impact on access to legal and illegal drugs and the predominant patterns of drug use. Preference for specific drugs and the patterns associated with their use that vary geographically across the United States and the world are of direct interest to physicians working in the armed forces. Social factors influencing drug preferences among substance users also vary considerably between communities within countries and between countries. To provide some context to drug and alcohol use in our community, students in the Multisystems and Complex Disease module were required to attend a local meeting of an Alcoholics Anonymous (AA) chapter or a meeting of a similar organization (e.g., Narcotics Anonymous), submit a brief written report, and then attend a small group discussion to share their thoughts on the experience. In this small group setting, students are asked to comment on their own reactions to the stories of people living with a substance use disorder, to examine their own biases relating to substance use disorders, to identify and explore the sources of their biases and reactions, and to consider the positive and negative implications of these biases with respect to the treatments they might offer to their patients. Student reaction to this class has generally been positive. Many students express surprise at the persons who they see attending these groups and the life histories that they hear. The comment “I was totally surprised; that person could have been my neighbor” is not uncommon in these groups. A majority of students write that the class has increased their understanding of individuals with a use disorder and their perceptions of the potential negative consequences of health care provider biases. A few students reported that they felt uncomfortable attending an AA session, but most reported that they were well received by the participants. (To avoid undue influence on the meetings, students were instructed that no more than two students from the class should attend any single AA meeting).
In addition, a lecture/discussion class was added in the Multisystems and Complex Disease module, in which legislation relating to drug scheduling and access as well as health care policy decisions that have affected self-administration of drugs are discussed. Other topics covered here include the association of life-threatening viral infections (human immunodeficiency virus, hepatitis C virus) with intravenous drug use and the very high costs of treating these infections. The potential for policy initiatives in this area to have unintended consequences that may exacerbate the problem is noted. The relationship between harm-reduction strategies (e.g., increased availability of naloxone to treat opioid overdoses, syringe and needle exchanges, or safe houses for injection of illicitly obtained drugs) and local declines in mortality and morbidity is also discussed.
Summary
We describe here an integrated approach to medical school instruction relating to the clinical use of opioid drugs and avoidance of opioid use disorder that was introduced as part of an overall revision of the preclinical curriculum at USU. Our approach has a few features that may be particularly appropriate for the unique role of this medical school but most features could easily be implemented at other schools. The emphasis is on an interdisciplinary approach in which the pharmacology of opioid drug actions is integrated with instruction from clinical psychologists, psychiatrists, and physicians from family medicine on practical issues associated with opioid use disorder and other substance use disorders in general. We have also included small group classes and other opportunities for student discussion of the issues, and we have expanded consideration of the social context relating to substance use disorders. In parallel with the changes in the preclinical curriculum, our clinical colleagues introduced a third-year “back to the basics” class in which students fresh from their internal medicine and psychiatry clerkships consider the clinical presentation and management of complex alcohol and opioid withdrawal cases in a panel discussion format with an internist, a psychiatrist, an emergency room physician, and a pharmacologist.
It is reasonable to propose that changing physician education practices concerning substance use disorders and the use of opioids for various pain conditions could be a useful tool for counteracting the opioid epidemic facing medical practice today. Unfortunately, we did not design this curriculum revision with a view to assessing outcomes in any quantitative manner. It was not feasible to have half the class take the “old” curriculum while the other half took the “new,” and lack of time and personnel prevented comparative evaluation of the effectiveness of some of the individual classes. Overall, our students performed better on pharmacology questions on the USMLE Step 1 examination in the years after the curriculum change (see Jurich et al., 2019), but many things beyond the substance use disorders curriculum had changed, and it is not possible to determine the effects of the curriculum change on responses to USMLE questions relating specifically to substance use disorders. It is challenging to evaluate the effects of preclinical instruction on physician prescribing practices many years later, in part because of the many other influences during the intervening period that may impact physician behaviors. One approach that might be applied in the future is to evaluate student retention of materials at later stages in the medical curriculum and to gather clinical preceptor perceptions of the knowledge, attitudes, and case management skills of residents and students during their clinical clerkships with respect to specific areas of the preclinical curriculum including pain management substance use disorders. These approaches would provide some information on the effectiveness of current teaching approaches but these are surrogate outcomes for the goal of optimizing prescribing practices at later points in the students’ careers, and the absence of precurriculum revision data in this context limits its usefulness if the goal is to show that the revised curriculum is superior to prior approaches.
The revised curriculum required a greater time commitment of the faculties of the pharmacology, medical and clinical psychology, psychiatry, medicine, and family medicine departments, but participating faculty members expressed increased satisfaction with the revised coverage of the topic. Medical student feedback has been limited. However, a subset of the class were regular attendees at all sessions including lectures, participated enthusiastically in the small group exercises, and expressed appreciation for the opportunity to consider more than the very basic pharmacology of opioids and other drugs. They were grateful to have an opportunity to learn in more depth than previously the complexity of the factors underlying this very challenging public health crisis.
Acknowledgments
An integrated curriculum cannot be developed without input and support from many people. We thank the following colleagues from USU for very important contributions to the development of the concepts underlying this revised curriculum and in the preparation and frequent updating of teaching materials: Drs. Fereshteh Nugent, Michael Schell, and Frank Shewmaker (Department of Pharmacology); Drs. Neil Grunberg, Andrew Waters, and Joanna Sells (Department of Medical and Clinical Psychology); Drs. Kelly Cozza, Eric Meyer II, Joshua Morganstein, and James “Curt” West (Department of Psychiatry); and Dr. Barbara Knollmann-Ritschell (Department of Pathology), Dr. Arnyce Pock (Associate Dean for Curriculum), and Dr. Francesca Cimino (Department of Family Medicine). In addition, we thank the directors of the Multisystems and Complex Diseases module, Drs. Angela Melton-Celsa and Christopher Jones, for making time in their module for the revised curriculum. We must also acknowledge the constantly changing group of faculty, residents, visiting fellows, clinical psychologists, and graduate students who have volunteered to serve as instructors for the small group classes for their support and commitment to the education of medical students.
Authorship Contributions
Wrote or contributed to the writing of the manuscript: Cox, Cote, Lucki.
Footnotes
- Received February 15, 2019.
- Accepted July 8, 2019.
The opinions or assertions contained herein reflect the private views of the authors. They should not be construed as official or reflecting the views of the U.S. Department of Defense or the Uniformed Services University of the Health Sciences.
↵1 Over the last 2 decades, the term “opioids” has gradually replaced the use of “opiates” in clinical and preclinical research publications as well as in the popular press. “Opioids” includes the older term “opiates,” which strictly speaking refers specifically to drugs derived from the opium poppy, Papaver sativa, like morphine itself. “Opioids” includes additionally synthetic and semisynthetic drugs that share the property of inducing useful therapeutic effects similar to those induced by morphine via activation of the μ-type opioid receptor. In addition to morphine and heroin, drugs like hydrocodone, oxycodone, fentanyl and its congeners, methadone, and meperidine, as well as endogenous peptides with morphine-like properties (e.g., enkephalins and endorphins), are all opioids. In this article, we use the term “opioids” in this broad context.
Abbreviations
- AA
- Alcoholics Anonymous
- CDC
- U.S. Centers for Disease Control and Prevention
- DSM
- Diagnostic and Statistical Manual of Mental Disorders
- USMLE
- U.S. Medical Licensing Examination
- USU
- Uniformed Services University
- U.S. Government work not protected by U.S. copyright




{kind=link}
{kind=link}
{kind=link}