Article Text

Abstract
Background: Natriuretic peptides have actions likely to ameliorate cardiac dysfunction. B-type natriuretic peptide (BNP) is indicated as treatment for decompensated cardiac failure.
Objective: To determine the utility of BNP in acute myocardial infarction (MI).
Design: Double-blind randomised placebo-controlled trial.
Setting: Tertiary hospital coronary care unit.
Patients: 28 patients with acute MI with delayed or failed reperfusion and moderate left ventricular dysfunction.
Interventions: Infusion of BNP or placebo for 60 hours after MI.
Main outcome measures: Neurohormonal activation and renal function in response to BNP infusion, secondary end points of echocardiographic measures of left ventricular function and dimension.
Results: BNP infusion resulted in a significant rise in BNP (276 pg/l vs 86 pg/l, p = 0.001). NT-proBNP levels were suppressed by BNP infusion (p = 0.002). Atrial natriuretic peptide (ANP) and NT-proANP levels fell with a significant difference in the pattern between BNP infusion and placebo during the first 5 days (p<0.005). C-type natriuretic peptide (CNP) and NT-proCNP levels rose during the infusion with higher levels than placebo at all measurements during the first 3 days (p<0.01). Cyclic guanosine monophosphate (cGMP) was raised during the infusion period showing a peak of 23 pmol/l on day 2 (placebo 8.9 pmol/l, p = 0.002), with a correlation between BNP and cGMP levels (p<0.001). Glomerular filtration rate (GFR) fell with BNP infusion but was not significantly lower than with placebo (71.0 (5.6) vs 75.8 (5.4) ml/min/1.73 m2, p = 0.62). Patients receiving nesiritide exhibited favourable trends in left ventricular remodelling.
Conclusions: Nesiritide, given soon after MI, induced increments in plasma cGMP and CNP and decrements in other endogenous cardiac peptides with a neutral effect on renal function and a trend towards favourable ventricular remodelling.
Statistics from Altmetric.com
Atrial natriuretic peptide (ANP) and B-type natriuretic peptide (BNP) released in response to cardiomyocyte stretch, are raised proportionately to intracardiac pressures and ventricular dysfunction.1–3 The natriuretic peptides induce natriuresis, suppression of the renin–angiotensin–aldosterone system and vasodilatation.4 5 ANP and BNP are sympatholytic and inhibit cardiac hypertrophy and fibrosis.6–9 These actions are likely to ameliorate cardiac dysfunction. Genetic manipulations leading to overexpression or blockade of the actions of the natriuretic peptides with disruption of either ANP or BNP or their common receptor lead to raised blood pressure or cardiac fibrosis, or both.7–9 BNP reduces ventricular filling pressures and relieves dyspnoea in patients admitted with decompensated heart failure.10–12 Actions upon renal function or neurohormones, or both, in clinical heart failure are less well established.13 Human recombinant BNP as “nesiritide” has FDA approval for administration to patients admitted with acutely decompensated heart failure.
Another potential therapeutic application of BNP or ANP, or both, is for early treatment after myocardial infarction (MI). Adverse left ventricular (LV) remodelling may be initiated soon after acute insults and natriuretic peptides may ameliorate this process. A single report indicates that administration of human ANP benefits LV remodelling after MI. Hayashi et al randomised patients with acute anterior ST elevation MI, to receive either intravenous nitrate or infusions of human ANP.14 At 30 days the group receiving ANP had less ventricular remodelling than the control group. There are no existing reports on the administration of nesiritide in the early post-MI period. We undertook a pilot study of the neurohormonal, haemodynamic, renal and echocardiographic effects of nesiritide given as a 60-hour infusion within 48 hours of MI.
METHODS
The trial protocol was approved by an ethics committee of the New Zealand Department of Health. All participants gave signed, informed consent.
Between December 2002 and August 2004, consecutive patients presenting with ST elevation MI with ventricular wall motion abnormality on echocardiography within 48 hours of onset of symptoms were screened. Inclusion criteria for the study included a first MI with typical clinical presentation, ST elevation (>2 mm elevation in two or more adjacent precordial leads, or >1 mm in adjacent limb leads) and a rise in plasma cardiac markers (creatine kinase rise to over twice the upper limit of normal), and elevation (with subsequent fall) of troponin T. Exclusions were inability to give informed consent, cardiogenic shock, blood pressure <100 mm Hg systolic or heart rate >100 bpm, or if unavailable for follow-up over 90 days. Twenty-eight patients met the trial criteria for inclusion and were enrolled into the study.
After initial acute management (thrombolytic and/or percutaneous coronary intervention plus drugs according to current best practice), patients received 60 hours of intravenous placebo (0.9% sodium chloride) or active nesiritide treatment (0.01 μgm/kg/min) according to a computer-generated random number. This dose is currently approved for administration in cases of decompensated heart failure. Infusion bags for nesiritide and placebo were indistinguishable and patients and investigators blinded to treatment. Additional drug treatment included antiplatelet agents, antilipid drugs, β-blockade and introduction of converting enzyme inhibitors according to current best practice.
Systolic, diastolic and mean arterial blood pressures together with heart rate and rhythm were serially recorded throughout the infusion and 2-day follow-up period. Plasma creatinine was measured daily during and after the infusion period and again at 30 and 90 days and glomerular filtration rates (GFRs) were estimated by both Cockcroft–Gault and MDRD (Modification of Diet in Renal Disease) equations.15 Blood for neurohormonal assays was collected before initiation of infusions and every 24 hours until day 5, and then again at 30 and 90 days. Venous blood was collected into EDTA and centrifuged immediately at 4°C with plasma stored at–80°C for later batched analysis to avoid interassay variability. Neurohormone measurements (ANP, NT-proANP, BNP, NT-proBNP, C-type natriuretic peptide (CNP), NT-proCNP, cyclic guanosine monophosphate (cGMP), plasma renin activity, plasma aldosterone, catecholamines, endothelin and adrenomedullin) were conducted by established immunoassays with intra- and interassay coefficients of variation within the range 3–9%.16 17
Echocardiography employed a Vingmed 3 machine (General Electric, Fairfield, Connecticut, USA) and was carried out by a single operator (RJH). The standardised imaging protocol included apical four- and two-chamber views according to the American Society of Echocardiography.18 Parasternal, short- and long-axis views (averaged over four cycles) were obtained for M-mode measurements of LV dimensions. LV volumes were calculated from apical four- and two-chamber views using the method of discs formula to provide LV end-systolic (LVESV), and end-diastolic (LVEDV) volumes. These were indexed according to body surface area for LVEDVi and LVESVi. Biplane diastolic and systolic volumes, and ejection fraction were calculated by planimetry according to Simpson’s method. Diastolic measures included mitral inflow E, A and DT pulse wave measurements. Tissue Doppler indices were collected from lateral and septal mitral annulus. E/E′ was calculated using the lateral E′. Regional wall motion scoring was performed according to the standard 16-segment American Society of Echocardiography model and indexed by dividing by the number of regions seen (RWMSi). The extent of coronary disease was assessed from coronary angiography by the Brandt jeopardy score.19 Primary end points included in-hospital and 30- and 90-day neurohormonal, haemodynamic, renal and echocardiographic effects. Clinical events were recorded.
Statistical analysis
The sample size reflects the intent to conduct a pilot study to test the feasibility of administering nesiritide in the acute MI setting and to provide initial information to allow design (including selection of study group sizes) of a full controlled trial with adequate power to assess possible effects on ventricular function at a later time. In addition, long-published experience from the investigators and others, of the neurohormonal, haemodynamic and renal effects of a range of infused doses of natriuretic peptides (including BNP) indicated a high likelihood of detecting clear neurohumoral effects at the dose employed. Data are presented as means (standard error). Serial measurements underwent analysis of variance with repeated measures with inspection for time by treatment interaction for comparison of the two treatment groups. A χ2 comparison of 3-month event rates between placebo and nesiritide groups was made. A p value <0.05 indicated significance.
RESULTS
Twenty-eight patients were randomised from 60 patients (47%) who met the enrolment criteria among a total of 220 patients screened for eligibility. Three had previously diagnosed ischaemic heart disease, 9 hypertension, 7 previously detected dyslipidaemia, 14 were ex- or current smokers and 10 had a family history of premature coronary artery disease. None of these background factors were significantly more prevalent in those randomised to receive nesiritide than in those receiving placebo. One patient died with myocardial rupture within 6 hours of enrolment and was used in baseline but not primary endpoint data. A second patient was excluded owing to violation of the enrolment criteria (creatine kinase rise less than twice the upper limit of normal). Twenty-seven were enrolled appropriately and twenty-six completed the trial. Groups were matched (table 1) with no significant difference in peak creatine kinase, baseline LVEF or RWMSi. Preinfusion neurohormonal, renal and haemodynamic measurements were similar. Primary angioplasty was performed in eight patients in the BNP group and nine receiving placebo (NS). Rates of angiography and angioplasty at any time during the duration of admission were equally high at 92% versus 91%. There was no significant difference in the Brandt score (9.58 (0.8) units in the nesiritide group and 9.48 (0.7) in the placebo group (p = 0.79)). The mean time from onset of infarction to the start of the infusion was 33 hours for BNP versus 34 hours for placebo (p = 0.87). Mean time to starting a β-blocker (19.7 (7.6) vs 11.4 (3.6) hours) or converting enzyme inhibitor (32.5 (3.6) vs 34.1 (9.1) hours) after the onset of infarction did not differ significantly (p = 0.41 and 0.86, respectively).
Neurohumoral responses
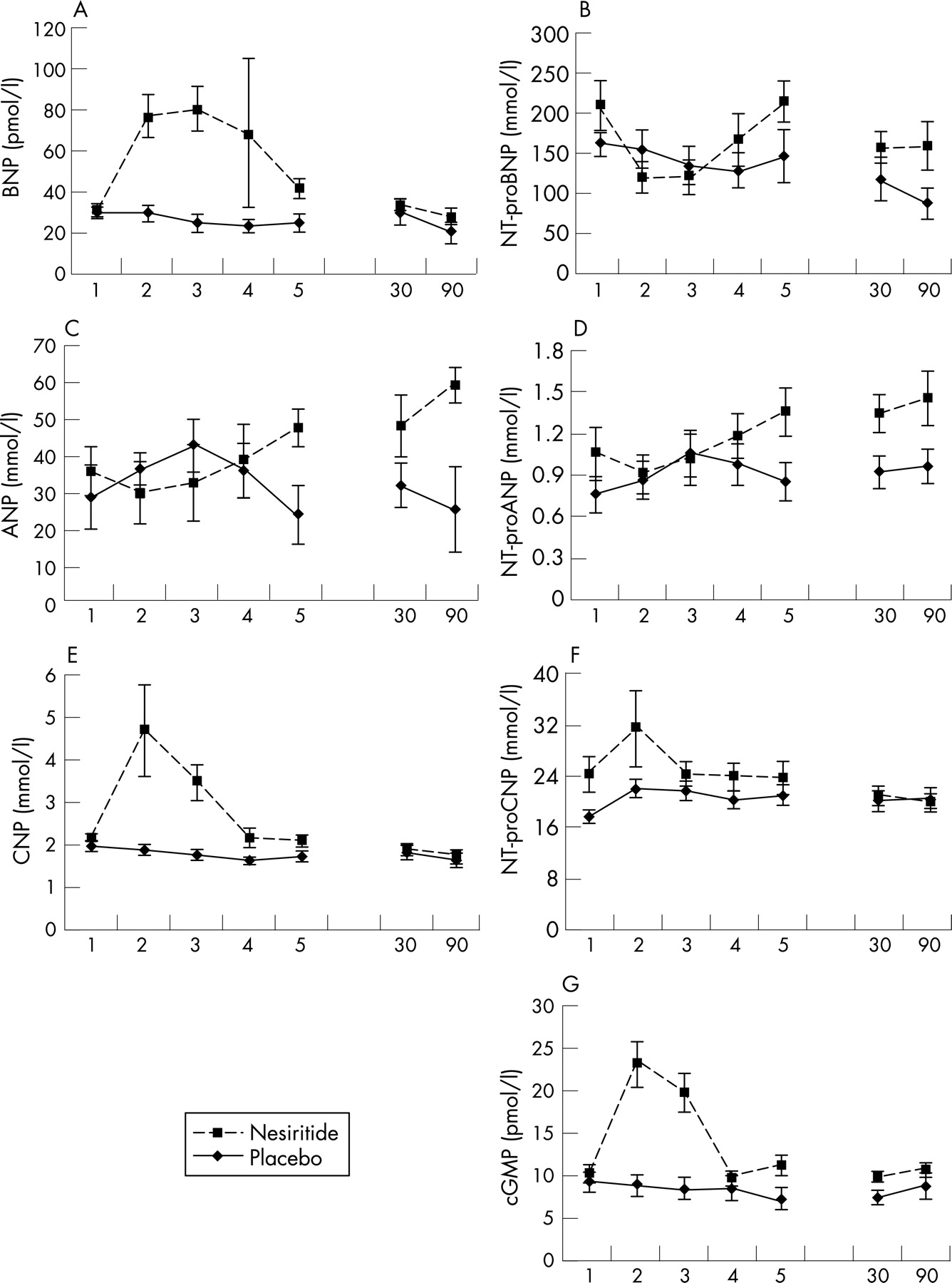
The initial plasma BNP level was about 100 pg/ml (29 pmol/l) in both groups (upper limit normal 40 pg/ml—that is, 12 pmol/l) with values declining in the placebo group over the following 5 days and an expected clear-cut increment (to above 250 pg/ml, ie. 72 pmol/l) during the course of nesiritide infusions (p<0.001; fig 1A). Plasma cGMP was raised above placebo group levels in parallel and proportionate to the increase in plasma BNP (p<0.001; fig 1G). Concurrent plasma concentrations of NT-proBNP and NT-proANP fell with the introduction of nesiritide infusions in contrast to stable or rising levels during administration of placebo (p<0.001; figs 1B and D). Plasma ANP levels did not differ significantly between groups (fig 1C). Plasma CNP was clearly augmented by BNP infusions (p<0.001; fig 1E), whereas its amino-terminal congener (NT-proCNP) rose subtly in both groups without a significant difference in the pattern of response (fig 1F). At 30 and 90 days plasma natriuretic peptide concentrations and cGMP levels did not significantly differ between groups.

Plasma renin activity was matched between the two groups except for a transient increment in renin in the nesiritide group on day 2 (table 2). There was no significant effect on serial aldosterone measurements. Nesiritide was associated with a non-significant trend towards an intrainfusion increment in plasma norepinephrine levels. Plasma adrenomedullin and endothelin concentrations did not differ between groups.
Heart rate and blood pressure
Heart rate was not significantly different between the two groups during the infusion (74.4 (3.2) vs 71.8 (2.1) bpm). Blood pressure was lower with nesiritide over the first 8–12 hours of infusions (BNP group 69.1 (1.9) vs 85.2 (3.8) mm Hg, p = 0.001) but pressures in the two groups were similar from 24 hours onwards.
Renal function
There was no significant difference in plasma creatinine (mean (SD)) for both placebo and active groups was 0.09 (0.02) mmol/l) or estimated GFR (placebo 72.9 (4.5) vs BNP 80.4 (5.3) ml/min/1.73 m2; p = 0.30) at enrolment. During nesiritide infusions there was a tendency for the GFR to fall but this was not significant when comparing preinfusion with mid-infusion values within the nesiritide group and was not significantly lower than placebo even at the point of apparent maximum separation between groups (BNP 71.0 (5.6) compared with placebo 75.8 (5.4) ml/min/1.73 m2; p = 0.62). Creatinine clearance was matched between the two groups before infusions, with a non-significant trend downwards in the nesiritide group during the latter part of infusions and return to closely matching postinfusion measurements on days 4 and 5. Measurements on days 30 and 90 matched.
Four (three receiving nesiritide and one placebo) patients exhibited a clear increase in plasma creatinine during the first 48 hours of infusions. In two (one receiving nesiritide and the other placebo) creatinine remained high at day 5 (ie, about 2 days after infusions ceased). However, in no case did day 30 or day 90 plasma creatinine remain raised above preinfusion levels. All four patients incurred large infarctions and became hypotensive concurrently with the acute decline in renal function. In one case the nesiritide infusion was halted at the time creatinine first rose. In two cases nesiritide was continued while angiotensin converting enzyme inhibitors were withdrawn for 1–2 days. In both these patients blood pressure rose and creatinine fell despite continuation of the peptide infusions.
Echocardiography
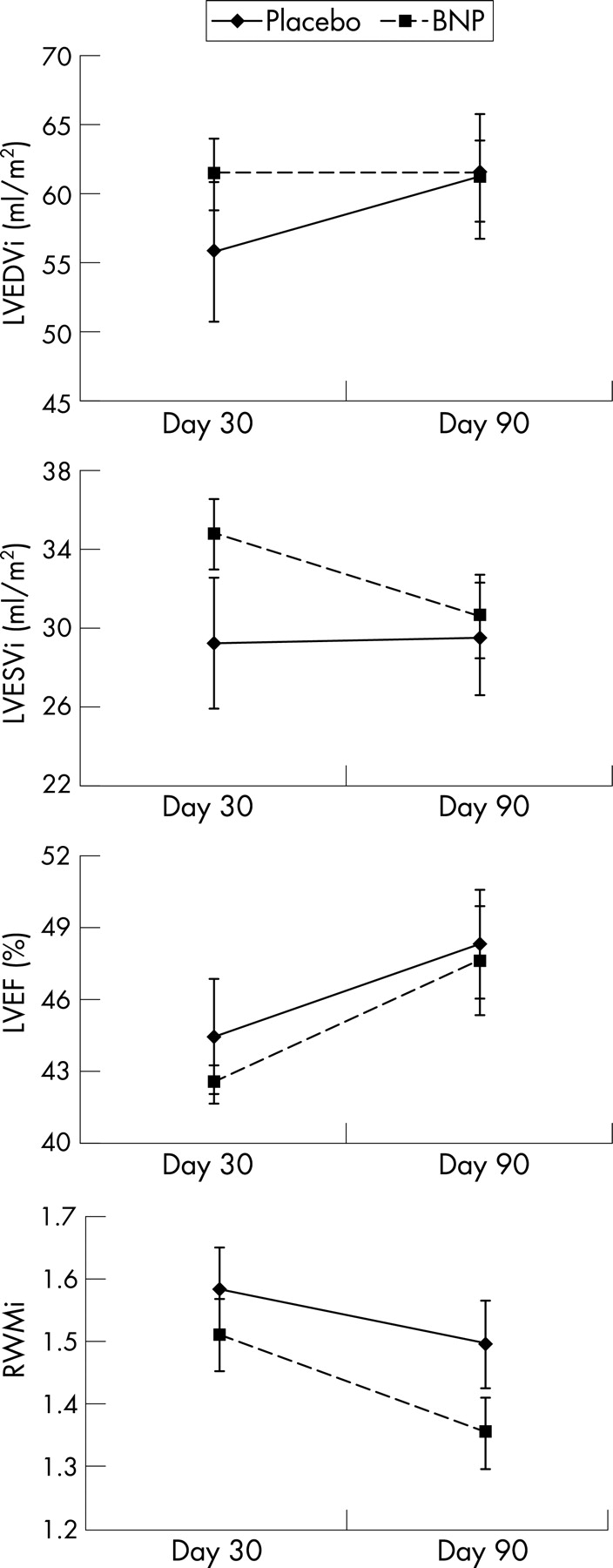
On days 1–5 no significant intergroup differences in left ventricular dimensions, LVEF, RWMSi or diastolic measurements were seen. Between days 30 and 90, LVEDV tended to increase (not seen in the group receiving nesiritide). LVESV tended to fall in the nesiritide group (absent with placebo), with a trend towards a greater fall in RWMSi (1.35 (0.06) vs 1.49 (0.07)—that is, less abnormality in the BNP group, p = 0.11) and greater increment in LVEF in the group receiving nesiritide over this later follow-up interval (fig 2). LVEF at day 5 correlated with subsequent change in LVEF to day 90 (r = −0.50, placebo and–0.89, nesiritide, with regression slopes differing significantly; p<0.001). That is, those with most impaired ejection fractions soon after MI exhibited the greatest increment in this measure by day 90, and this pattern was significantly more apparent in the nesiritide group.

{kind=link}
{kind=link}
Adverse events
A death from myocardial rupture occurred with placebo. Inpatient hypotensive and renal events were as outlined above. There were no additional deaths or recurrent MI between discharge and 90 days. Two patients in each group developed clinically apparent LV failure, deemed to necessitate diuretic treatment, during their inpatient stay. Major adverse cardiac event rates did not differ significantly between groups.
DISCUSSION
As far as we know, this is the first report of the neurohormonal, haemodynamic, renal and echocardiographic effects of nesiritide infused soon after MI. Infusions of nesiritide induced increments in plasma BNP within the range observed in severe MI and in heart failure.20–23 Concurrent falls in plasma NT-proBNP and proANP suggest a reduction of intracardiac pressures, with consequent reduction in secretion of endogenous natriuretic peptides. It is also possible that nesiritide exerted a negative feedback upon endogenous peptide secretion through natriuretic peptide receptors.24 The neutral effect on plasma ANP levels may reflect the net result of reduction in secretion combined with competition for clearance. The reduced release of endogenous peptide was not sufficient to offset the additional bioactivity induced by the nesiritide as shown by the increment in circulating plasma cGMP (second messenger) levels.
This is the first report of increments in plasma CNP during nesiritide infusions. CNP differs from both ANP and BNP in that it is not a predominantly cardiac product but rather is produced from the vascular endothelium throughout the body.25 It is released from the endothelium, predominantly abluminally, to induce vasodilatation via a relaxant effect upon vascular smooth muscle cells of the vascular media.26 It shares clearance pathways with ANP and BNP including the NPR clearance receptor and cleavage by neutral endopeptidase 24.11. Plasma concentrations of both CNP and NT-proCNP are raised in human heart failure.27 The increment in plasma CNP without a similar effect on NT-proCNP levels suggests competition specifically for clearance of the C-terminal peptides, ANP, BNP and CNP. This has been demonstrated experimentally in both animals and in human beings receiving combined infusions of these peptides.28 29 This new finding raises the possibility that a proportion of the vascular effects of infused nesiritide may be secondary to induction of higher circulating and tissue levels of CNP.
In contrast to the consistently observed suppression of renin activity and plasma aldosterone in normal humans receiving physiological doses of either ANP or BNP,4 5 no such effect was seen in the current study. Early infusion renin activity was briefly increased. The cause for this is uncertain. Possibly, the subtle blood pressure reduction induced by BNP coupled with variable drug effects was sufficient to induce a short-lived intergroup difference in plasma renin activity in opposition to the known primary renin-suppressant action of BNP. Notably, there was no parallel short-term increment in plasma aldosterone.
Noradrenaline exhibited a trend towards increases above placebo levels during nesiritide infusion. This might reflect a sympathetic response to the small fall in blood pressure induced by BNP, but it was subtle and did not achieve statistical significance. Notably, heart rate was not affected by the BNP infusion. A relative lack of baroreceptor-mediated increase in heart rate is a repeated observation in the course of relatively low-dose natriuretic peptide infusions.6 In addition, the introduction of β-blockade in the vast majority of patients in both subgroups would tend to blunt any heart rate response.
The possible adverse effects of nesiritide infusions in excess of 24 hours’ duration upon renal function, has been the subject of a recent report, attracting editorial comment in leading periodicals.13 A meta-analysis of five double-blind, randomised controlled trials of nesiritide infused for periods of 24 hours or more in a total of 1269 patients with decompensated heart failure consistently showed an increased risk of a rise in creatinine of more than 0.5 mg/dl (44 μmol/l; risk ratio 1.54 (1.19 to 1.98); p<0.001).13 However, no continuing measurements of renal function were reported and it is unknown whether this pattern presaged a permanent reduction in renal function or was associated with adverse cardiovascular prognosis. In the current study, nesiritide was associated with a non-significant reduction in calculated GFR in the immediate peri-infusion period (up to day 5), which was no longer apparent at 30 and 90 days’ follow-up. Examination of individual cases in the current pilot trial suggested declines in renal function reflected severe MI and were not specific to administration of nesiritide. This topic requires further consideration in larger trials, and notably, a current trial being conducted under the aegis of the European Medicines Association will test nesiritide in a randomised controlled trial of 1900 patients with decompensated heart failure and will include careful follow-up of renal effects and mortality up to 6 months.
Echocardiography, soon after infarction, demonstrated no differences between groups. In view of multiple events, including introduction of multiple powerful cardiovascular drugs and the expected wide interindividual variation in response to acute MI, this is not surprising. In the later follow-up period up to 30 and 90 days when drug treatment has been established, acute events have abated and a more gradually evolving remodelling process can be expected to occur. Although by no means definitive, the comparison between our two groups showed a trend towards a difference in ventricular remodelling patterns between 30 and 90 days. While LVEDV remained unchanged in the nesiritide group, it tended to rise in the placebo group, whereas the opposite pattern was true for LVESV which fell in the actively treated group and remained static in the placebo group. In addition, there was a trend towards greater improvement in RWMSi in the group receiving BNP. Furthermore, the pattern of greater increments in LVEF between days 5 and 90 in those with greatest initial impairment was significantly more apparent in the nesiritide group, suggesting that those with greatest early post-MI impairment may be most likely to benefit from nesiritide.
How a 60-hour, postinfarction, infusion of BNP might affect ventricular remodelling over 90 days after MI is uncertain. Remodelling may begin within hours of MI with an array of processes set in train, including cardiomyocyte lengthening, infarct thinning or expansion, inflammation and interstitial changes.30 Possibly, BNP can modify one or more elements in the early phase of this process, resulting in altered or reduced ventricular remodelling becoming apparent 1 to 3 months later.
In summary, this pilot study demonstrates that administration of nesiritide soon after MI induces clear increments in plasma BNP with parallel increments in plasma cGMP levels and concurrent reductions in endogenous NT-proBNP and proANP but sharp increases in CNP. Effects on blood pressure were mild. Symptomatic hypotension occurred in two cases. Effects on other neurohormones were subtle and not significant or sustained. Estimates of renal function suggest a mild trend towards reduced glomerular filtration only while infusions are in progress with no suggestion of sustained decrements in renal function at up to 90 days’ follow-up. These pilot results encourage further trials adequately powered to test the potential benefit of early postinfarction BNP infusions upon later ventricular remodelling and to assess more fully potential short- and long-term effects on both renal function and cardiovascular outcomes.
Acknowledgments
This study received support from a New Zealand Health Research Council grant. AMR is the New Zealand National Heart Foundation professor of cardiovascular studies. Scios Incorporated is a Johnson & Johnson company, which supplied the nesiritide free of charge.
REFERENCES
Footnotes
-
Funding: Scios Incorporated is a Johnson and Johnson company which supplied the nesiritide free of charge. Scios Inc was not involved in the design, execution, analysis, or reporting of this trial.
-
Competing interests: None.
-
Ethics approval: Approved by an ethics committee of the New Zealand Department of Health.