


Abstract
Animal models of pulmonary inflammation are critical for understanding the pathophysiology of asthma and for developing new therapies. Current conventional assessments in mouse models of asthma and chronic obstructive pulmonary disease rely on invasive measures of pulmonary function and terminal characterization of cells infiltrating into the lung. The ability to noninvasively visualize and quantify the underlying biological processes in mouse pulmonary models in vivo would provide a significant advance in characterizing disease processes and the effects of therapeutics. We report the utility of near-infrared imaging agents, in combination with fluorescence molecular tomography (FMT) imaging, for the noninvasive quantitative imaging of mouse lung inflammation in an ovalbumin (OVA)-induced chronic asthma model. BALB/c mice were intraperitoneally sensitized with OVA-Alum (aluminum hydroxide) at days 0 and 14, followed by daily intranasal challenge with OVA in phosphate-buffered saline from days 21 to 24. Dexamethasone and control therapies were given intraperitoneally 4 h before each intranasal inhalation of OVA from days 21 to 24. Twenty-four hours before imaging, the mice were injected intravenously with 5 nmol of the cathepsin-activatable fluorescent agent, ProSense 680. Quantification by FMT revealed in vivo cysteine protease activity within the lung associated with the inflammatory eosinophilia, which decreased in response to dexamethasone treatment. Results were correlated with in vitro laboratory tests (bronchoalveolar lavage cell analysis and immunohistochemistry) and revealed good correlation between these measures and quantification of ProSense 680 activation. We have demonstrated the ability of FMT to noninvasively visualize and quantify inflammation in the lung and monitor therapeutic efficacy in vivo.
Asthma is a chronic inflammatory disease of the airways characterized by a T cell-driven eosinophil and mast cell inflammation that leads to intermittent, reversible airway obstruction. For many patients, the disease has its roots in infancy, and both genetic (Cookson, 1999) and environmental factors (viruses, allergens, and occupational exposures) (Venables and Chan-Yeung, 1997; Halonen et al., 1999; Stein et al., 1999) contribute to its inception and progression. Asthma is a rapidly growing public health problem affecting 300 million people worldwide (Braman, 2006), and it continues to be a major cause of morbidity. Because of the prevalence of asthma and the complexity of this multifactorial and multicellular disease, it has become important to establish relevant animal models to better aid in the discovery of therapeutic agents.
Preclinical research using animal models of pulmonary inflammation has been critical for understanding the pathophysiology of asthma and for developing new therapies, and a variety of mouse models of asthma have been developed that capture specific inflammatory mechanisms of asthma (Bice et al., 2000). In normal healthy animals, it is necessary to immunize and challenge the mice with specific antigens (Zhou et al., 1998; Campbell et al., 1999; Clarke et al., 1999; Tournoy et al., 2000) to induce allergic asthma-like pulmonary inflammation. These types of animal models have helped to establish asthma as a unique form of chronic airway inflammation involving lymphocytes, mast cells, and eosinophils. Among these, eosinophils are the predominant effector cells for tissue damage and pulmonary dysfunction (Seminario and Gleich, 1994; Rankin et al., 2000), and airway eosinophil influx correlates well with the severity of airway hyperreactivity (Hamelmann et al., 1997; Hogan et al., 1997; Wills-Karp, 1999). Once eosinophils have infiltrated the lung, numerous inflammatory changes in the airways are triggered, including the release of a wide variety of immunomodulatory molecules, which can directly damage airway epithelium, cause degranulation of basophils and mast cells (Wills-Karp, 1999), and prime the lung for subsequent occurrences of allergic pulmonary inflammation (Rankin et al., 2000; Busse and Lemanske, 2001).
Researchers using such established mouse models of asthma currently rely on invasive measures of pulmonary function and ex vivo characterization of pulmonary cellular infiltration. Although these assessments of disease status are used extensively and highly validated, they are terminal procedures that preclude the possibility of repeated, longitudinal assessment of test subjects. In contrast, optical in vivo imaging of live animals provides a tool for noninvasive repeated assessments of in situ biological processes, but it is not yet validated as a widespread metric in asthma research. Recent advances in photonic technology have taken optical imaging beyond the standard, qualitative two-dimensional fluorescence reflectance imaging (FRI) into the realm of three-dimensional fluorescence molecular tomography (FMT) imaging for localization and quantification in deep tissue. The pairing of powerful, deep-tissue FMT imaging with appropriate near-infrared (NIR) imaging agents allows the detection and quantification of important biological processes, such as cellular protease activity, vascular leak, and receptor up-regulation, by accurately reconstructing the in vivo distribution of systemically injected NIR imaging agents. FMT has been effectively used to image tumors (Weissleder and Ntziachristos, 2003; Montet et al., 2005; Deguchi et al., 2006), atherosclerosis (Chen et al., 2002; Weissleder and Ntziachristos, 2003; Montet et al., 2005; Deguchi et al., 2006), and cardiac pathologies (Nahrendorf et al., 2007; Sosnovik et al., 2007).
A recent publication (Cortez-Retamozo et al., 2008) showed that optical tomographic imaging of secreted matrix metalloprotease (MMP)-12 activity can be an effective tool for assessing the severity of ovalbumin-induced pulmonary eosinophilia and matrix remodeling. In contrast, for our studies, we imaged a cathepsin-activatable agent (ProSense680; VisEn Medical, Inc., Bedford, MA) because cathepsins are active in intracellular lysosomes of inflammatory eosinophils, providing intracellular accumulation of the imaging agent and, thus, a more selective quantification of eosinophils. Efforts to cross-validate asthma-induced cathepsin activity with standard bronchoalveolar lavage (BAL) cell counts and ex vivo lung histology showed excellent cell internalization and good correlations with eosinophil counts. Because steroids are currently the most effective treatment for asthma (Rankin et al., 2000; Busse and Lemanske, 2001), we also determined the sensitivity of optical tomography and ProSense 680 to accurately assess therapeutic intervention (with a range of dexamethasone treatment doses). The use of FMT imaging in asthma research could provide better, noninvasive tools for understanding pulmonary inflammation and to help develop new therapeutics.
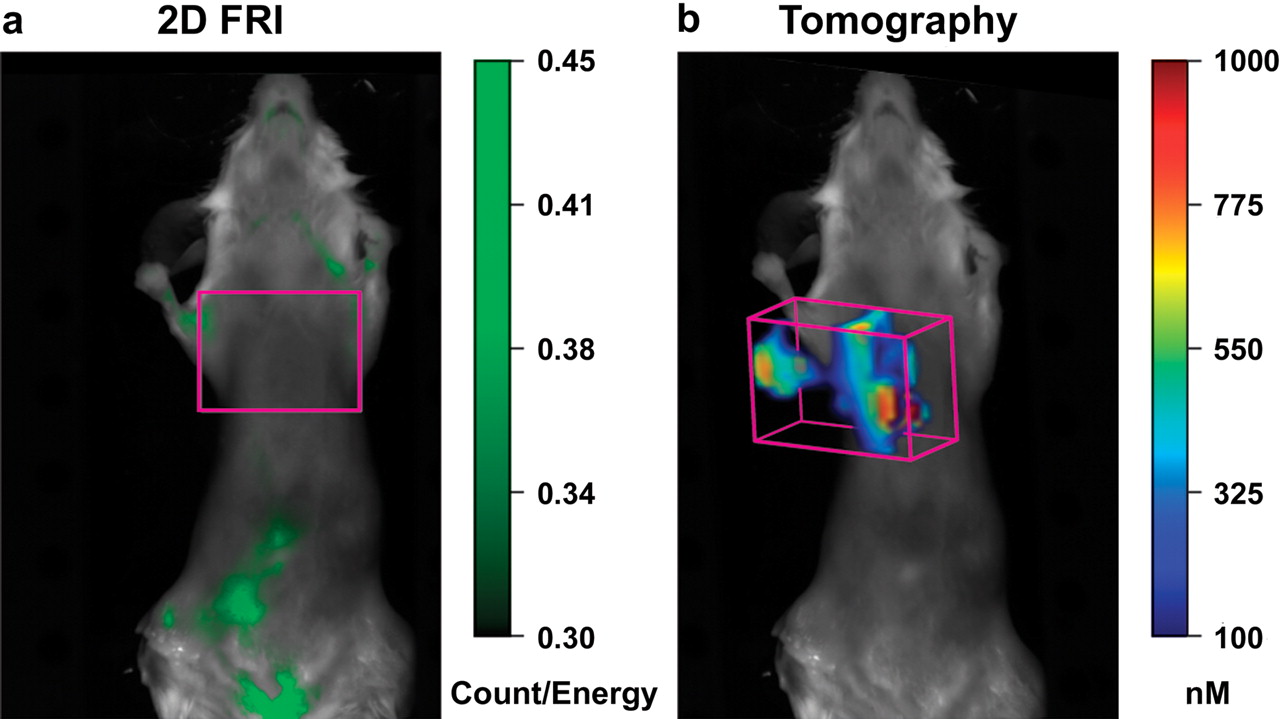
Tomographic detection of lung inflammation. Female BALB/c mice received intraperitoneal immunization with 50 μg of OVA/2 mg of Alum (days 0 and 14) followed by four intranasal challenges with 100 μg of OVA (days 21–24). ProSense 680 (5 nmol/mouse) was injected intravenously 4 h after the last intranasal challenge, and imaging was performed 24 h later using the VisEn FMT 2500 in vivo imaging system. FRI (a) showed some epifluorescent signal in the abdominal region but no apparent fluorescence in the upper torso lung region (purple square). In contrast, tomographic imaging of the same mouse (b) revealed extensive fluorescence within the lungs (purple box) attributed to pulmonary inflammation.
Materials and Methods
Experimental Animals. Specific pathogen-free female BALB/c mice (6–8 weeks of age, 18–20 g) were obtained from Charles River Laboratories, Inc. (Wilmington, MA) and housed in a controlled environment (72°F; 12-/12-h light/dark cycle) under specific pathogen-free conditions with water and food provided ad libitum. All experiments were performed in accordance with VisEn Institutional Animal Care and Use Committee guidelines for animal care and use.
Asthma Induction Protocol. BALB/c mice were immunized on days 0 and 14 by intraperitoneal injections of 50 μg of OVA (grade V; Sigma-Aldrich, St. Louis, MO) together with 2 g of aluminum hydroxide (alum; Sigma-Aldrich) in phosphate-buffered saline (PBS). Control mice received intraperitoneal injections of PBS. From days 21 to 24, both immunized and control mice were given daily intranasal administration of 100 μg of OVA (grade VII; Sigma-Aldrich) solubilized in PBS.
Analysis of BAL Inflammatory Cells. BAL cell analysis in OVA-challenged and control mice was performed 24 h after the last intranasal OVA challenge. Mice were killed by CO2 inhalation, and a midline neck incision was made to cannulate the trachea. The lungs were washed three times with 0.8 ml of lavage buffer PBS containing 1% fetal calf serum and 2% paraformaldehyde (Poly Scientific, Bay Shore, NY), the recovered BAL cell suspension was centrifuged at 300g for 10 min at 4°C, and cells were resuspended in 0.5 ml of lavage buffer. Cells were counted on a hemocytometer, and cytospin preparations of 2 × 105 cells were used to establish differential cell subpopulation counts (Hemacolor staining system; EMD Biosciences, San Diego, CA).
Fluorescent Agents for the Detection of Inflammation. A commercially available cathepsin-activatable NIR imaging agent, a fluorophore-conjugated graft copolymer of polyethylene glycol and poly(Lys) (ProSense 680; VisEn Medical, Inc.), was used via intravenous administration in all imaging studies. The typical adult mouse dose is 2 nmol in 150 μl of saline, but for these studies, a higher dose of 5 nmol/mouse was used to enhance pulmonary distribution and signal.
In Vivo FMT 2500 Tomographic Imaging and Analysis. OVA-challenged and control mice were injected intravenously with ProSense 680 on day 24 (i.e., 4 h after the last intranasal administration of OVA-Alum). On day 25, mice were anesthetized using an intraperitoneal injection of ketamine (100 mg/kg) and xylazine (20 mg/kg) and depilated to minimize fur interference with fluorescent signal. Nair lotion (Church and Dwight Co., Inc., Princeton, NJ) was applied thickly on skin over the upper torso (front, back, and sides) of each mouse, rinsed off with warm water, and reapplied until all fur had been removed. OVA-challenged and control mice were then imaged using the FMT 2500 fluorescence tomography in vivo imaging system (VisEn Medical, Inc.). In brief, the anesthetized mice were carefully positioned in the imaging cassette, which was then placed into the FMT imaging chamber. An NIR laser diode transilluminated (i.e., passed light through the body of the animal to be collected on the opposite side) the thorax region, with signal detection occurring via a thermoelectrically cooled charge-coupled device camera placed on the opposite side of the imaged animal. Appropriate optical filters allowed collection of both fluorescence and excitation data sets, and the multiple source-detector fluorescence projections were normalized to the paired collection of laser excitation data. The entire image acquisition sequence took approximately 4 to 5 min per mouse. FMT 2500 FRI was routinely performed before each tomographic imaging session using built-in LED front illuminators and collection of single-camera images. For some animals, these whole-body FRI images were represented as controls for tomographic data sets.
FMT Reconstruction and Analysis. The collected fluorescence data were reconstructed by FMT 2500 system software version 1.1 (VisEn Medical, Inc.) for the quantification of three-dimensional fluorescence signal within the lungs. Three-dimensional regions of interest were drawn in the upper torso encompassing the lung region (below the manubrium and above the liver), excluding 2 mm ventrally and 3 mm dorsally. A threshold was applied identically to all animals that was equal to 2× the mean lung fluorescence of the control mice. This minimized the quantification of the low-intensity, widespread background fluorescence due to activation of ProSense 680 by normal resident lung macrophages but allowed optimal detection of high fluorescent signal in activated eosinophils. The total amount of lung fluorescence (in picomoles) and the fluorescence volume (in millimeters cubed) were automatically calculated relative to internal standards generated with known concentrations of appropriate NIR dyes. For visualization and analysis purposes, FMT 2500 system software provided three-dimensional images.
Ex Vivo Tissue Imaging. To confirm that the fluorescent signal in OVA-challenged mice originates in the lungs, NIR fluorescent images of excised lung tissues were captured using a 2-min acquisition with a monochrome charge-coupled device camera equipped with an emission long-pass filter at 700-nm wavelength (Kodak Image Station 2000 mm; Carestream Health, Rochester, NY). Relative fluorescence unit intensity and distribution in lung tissues were performed by the Kodak system software, with ratios established by comparing tissue fluorescence with the background fluorescence of the image field. In some experiments, lungs were carefully dissected to separate the five lobes of the lung, washed with PBS, and imaged ex vivo by FRI to provide high-resolution images of probe distribution in the major airways.
Steroid Treatment. Dexamethasone (Sigma-Aldrich), a very potent glucocorticoid for controlling lung inflammation, was prepared as a suspension in PBS, and 100 μl was injected intraperitoneally (0.03, 0.3, and 3 mg/kg) 4 h before each daily intranasal OVA administration on days 21 to 24.
Fluorescence Microscopy. BAL cells from OVA-challenged and control mice receiving an intravenous injection of ProSense 680 were fixed with 2% paraformaldehyde for 30 min at 4°C. The cells were pelleted by centrifugation, and excess fixative was removed. The cells were resuspended in 0.5 ml, counted, and smeared onto microscopy slides (2 × 105 cells/smear). The slides were allowed to air dry in the dark, mounted with ProLong Gold antifade reagent with 4,6-diamidino-2-phenylindole (Invitrogen, Carlsbad, CA), and cured overnight at 4°C in the dark. Merged images of the nuclear staining (4,6-diamidino-2-phenylindole) and Cy5.5 signals were collected using fluorescence microscopy (Carl Zeiss MicroImaging, Inc., Thornwood, NY) with appropriate optical filters. Nuclear morphology was used to identify eosinophils and to determine their uptake and activation of ProSense 680.
Statistical Analysis. The statistical significance of differences between experimental groups was analyzed using one-tailed analysis of variance. Group means were compared using the Scheffé multiple comparison test, with p values < 0.05 considered significant.
Results
OVA-Challenged Mice Show High Activation of a Cathepsin-Activatable Agent in Vivo. To assess the relative benefit of quantitative tomographic imaging compared with standard two-dimensional FRI, we imaged OVA-induced pulmonary inflammation using both types of imaging technology. ProSense 680 was selected for imaging, an agent that is activated in vivo predominantly by a family of lysosomal cathepsin proteases. Intravenous injection of ProSense 680 allows the detection of activated macrophages, eosinophils, and neutrophils. FRI of OVA-challenged mice revealed only low levels of fluorescent signal predominantly in the lower abdomen (Fig. 1a), attributed to bladder and intestine, and showed little or no fluorescence in the animals' lung regions. In contrast, FMT imaging of the thorax region of OVA-challenged mice revealed deep-tissue fluorescence associated with the disease process (Fig. 1b). The signal provided a clear three-dimensional image indicating the presence of widespread lung protease activity with apparent intrapulmonary heterogeneity of signal. Surgical exposure of the thoracic cavity confirmed the presence of fluorescence within the chest and that this fluorescence was solely localized within the lung tissue (data not shown). FMT imaging of multiple animals (Fig. 2a) shows a consistent pattern and extent of fluorescence expression in OVA-challenged mice, with control animals showing much lower levels of fluorescence, attributed to normal resident macrophages. It is important that noninvasive tomographic fluorescence imaging not only detected disease-related protease activity, rendering striking deep-tissue images, but also allowed the accurate quantification of this fluorescence. FMT measured a 10-fold increase in ProSense 680 fluorescence in the lungs of OVA-challenged mice (>120 pmol/lung) compared with those of control mice (<10–15 pmol/lung) (Fig. 2b). In addition, the FMT software precisely quantified the volume of the fluorescence within the lung regions of the mice to provide a measure of affected lung volume, showing approximately a 5-fold increase in OVA-challenged animals compared with controls (∼375 mm3 in OVA-challenged mice versus 75 mm3 in controls). Both the total fluorescence quantification (picomoles) and the volume measurement showed high statistical differences in comparing OVA-challenged and control mice (p < 0.003).

Quantification of pulmonary inflammation. OVA-challenged BALB/c mice show a consistent pattern and magnitude of lung fluorescence after ProSense 680 administration, whereas control mice (receiving only intranasal saline) show minimal fluorescence in their lungs (a). Three-dimensional regions of interest were placed within the lung regions (purple boxes) of OVA-challenged and control mice to establish the appropriate regions for fluorescence quantification. Tomographic analysis (b) shows high amounts (total picomoles per lung ± S.E.M.) and higher volume (millimeters cubed ± S.E.M.) of ProSense 680 fluorescence within the lung region of OVA-challenged mice, with minimal fluorescence measured within control lungs.

Ex vivo tissue imaging: excised lung tissues from representative OVA-challenged and control mice were assessed for ProSense 680 fluorescence intensity using a color scale to indicate relative fluorescence units (RFU) (a). Images revealed significant inflammation-related increases (mean tissue/background fluorescence ratio ± S.E.M.) (p < 0.05) in lung fluorescence intensity (b). These changes in ex vivo fluorescence ratio confirmed the dramatic increase in fluorescence signal in the lungs quantified by tomographic imaging. The figure is representative of four separate studies (n = 5 mice/group). Asterisks indicate statistical significance (***, p < 0.001).
Cathepsin Activity in Inflamed Lungs Shows Predominant Airway Distribution. Ex vivo tissue FRI was performed to confirm that the fluorescent signal originated specifically from the lung, supporting the noninvasive in vivo FMT 2500 imaging results. Excised lungs from sacrificed mice showed widespread fluorescence throughout the lung, whereas control lungs showed minimal fluorescence (Fig. 3a). Measurement of the ratio of fluorescence intensity in OVA-challenged lungs yielded signal intensity >5-fold higher than that in lungs of control mice (Fig. 3b). It is notable that the profile of fluorescence ratios for the excised lungs, comparing OVA-challenged and control mice, corresponded well with the noninvasive quantification performed by FMT 2500. High-magnification inverted grayscale FRI images of individual lung lobes (Fig. 4a) further reveal a very clear and predominant distribution of activated ProSense 680 in the inflamed bronchial tree of OVA-challenged lungs, with some lower signal also seen distributed throughout the lung tissue. In comparison, control lungs showed very little signal in either the parenchymal or bronchial regions and were unable to be represented as inverted grayscale images (not shown). BAL cell differential analysis indicates the expected recruitment of a predominant and large number of eosinophils (>60% of the total cells) infiltrating the airways of OVA-challenged mice, with no detectable eosinophils in control mice (Fig. 4b). It is of interest to note that BAL cells contribute less than half of the overall lung fluorescence, as determined by imaging lungs before and after lavage (data not shown), suggesting that noninvasive imaging may provide the best means of quantifying all inflammation occurring in the lungs of OVA-challenged mice.
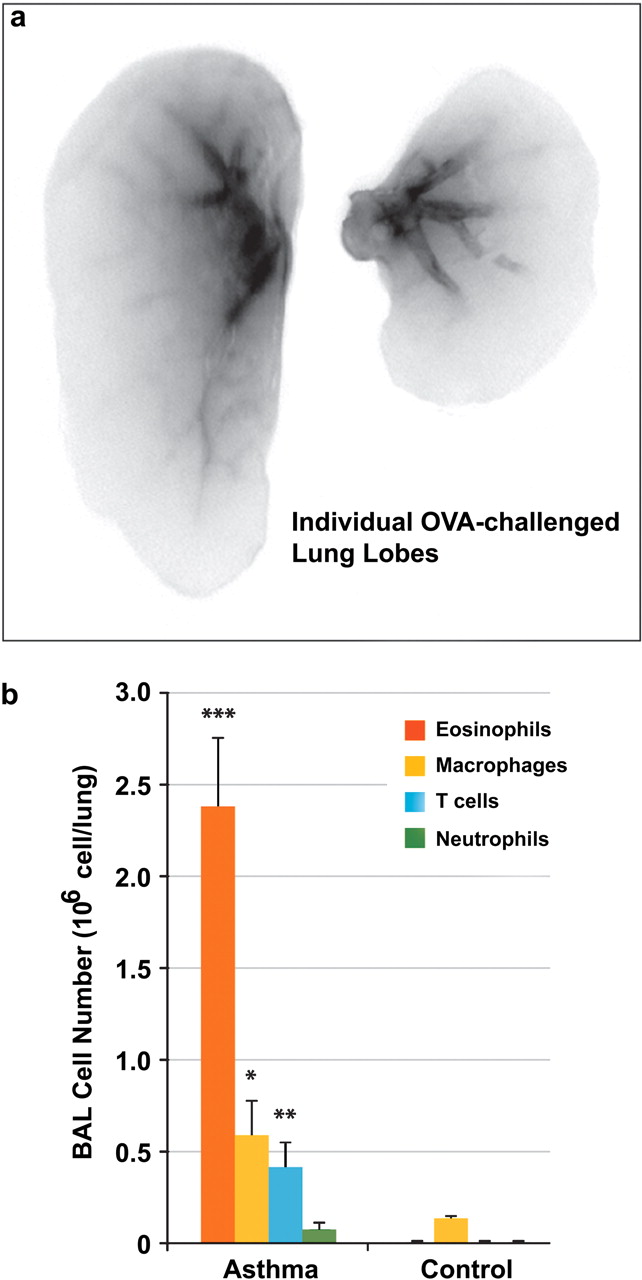
Ex vivo lung and BAL assessment: a high-magnification inverted grayscale FRI image of two lung lobes from a representative OVA-challenged mouse (a) shows the predominant distribution of activated ProSense 680 (black) in the inflamed bronchial tree, with some lower signal (gray) also seen distributed throughout the lung tissue. In comparison, control lungs showed very little signal and could not be represented as inverted grayscale images (data not shown). BAL cells of OVA-challenged mice (b) show a predominance of eosinophils taking up and activating ProSense 680, with few eosinophils and little or no detectable fluorescence in BAL cells from control mice. Asterisks indicate statistical significance (*, p < 0.05; **, p < 0.01; ***, p < 0.001).
Eosinophils Show High Cathepsin Activity in Inflamed Lungs. Frozen tissue sections taken from the lungs of OVA-challenged mice demonstrated multiple areas of fluorescence localized throughout the lung compared with the minimal fluorescence detectable in control lungs (Fig. 5a), in strong agreement with ex vivo and in vivo imaging results. Fluorescent microscopy of the BAL cells isolated from OVA-challenged and control mice that received intravenous ProSense 680 injection further established that the eosinophils were the predominant cell activating ProSense 680 fluorescence in the airways (Fig. 5b). BAL mononuclear cells in the same mice showed little or no fluorescence, and the small number of collected BAL cells from control mice, predominantly macrophages, showed minimal fluorescence.
Inhibition of Cathepsin Activity in Inflamed Lungs by Dexamethasone Correlates with BAL Eosinophils. To evaluate whether the effect of a conventional treatment could be detected and quantified noninvasively by FMT imaging, mice were treated with dexamethasone and then imaged by FMT. Images acquired by FMT showed high fluorescence signal in the lung regions of untreated OVA-challenged mice compared with those of controls (Fig. 6a) and an apparent dose-dependent decrease in fluorescence. Tissue FRI images (Fig. 6b) showed definite effects of treatment on ProSense 680 lung signal, with the signal remaining fairly widespread at the lowest treatment dose and near the level of control lungs at the high dexamethasone dose. The fluorescence quantified by FMT in dexamethasone-treated mice decreased in a dose-dependent fashion, showing 55, 65, and 80% inhibition at 0.03, 0.3, and 3 mg/mouse dose, respectively (Fig. 7a). In addition, the volume of the fluorescent signal, an indicator of the volume of the lung affected by inflammation, changed with dexamethasone dose; treated mice showed a 33% decrease in the volume of lung fluorescence at 0.3 mg/kg dexamethasone and a 53% decrease at 3 mg/kg. The ED50 of dexamethasone in this asthma model was calculated as approximately 0.02 mg/kg when using the total lung ProSense 680 pmol readout, whereas the ED50 was approximately 2 mg/kg by fluorescence volume (a measure of the extent of affected lung). This was an expected and useful finding because it indicated that although disease was decreased by 80%, low-grade inflammation remained more widespread. Overall, the dexamethasone effects on BAL eosinophilia were profound (Fig. 7b) and achieved approximately 90% inhibition of BAL eosinophil numbers at the highest two doses of steroid (ED50, ∼0.04 mg/mouse). These cell counts correlated well with FMT quantification (Fig. 7c). In addition, tissue FRI ratios correlated well with in vivo FMT quantification (r2 = 0.97); however, this method proved roughly 5-fold less sensitive at detecting therapeutic effects (ED50, ∼0.4 mg/mouse). This treatment clearly study showed tremendous inhibition of eosinophilia, and the addition of ProSense 680 imaging further provided information on the distribution and volume of the eosinophilia in vivo and ex vivo.

Ex vivo lung and BAL assessment: frozen lung tissues from representative OVA-challenged and control mice (a) were sectioned and assessed by fluorescence microscopy to detect regions of ProSense 680 activation within the tissue, revealing significant fluorescence in lung tissue from OVA-challenged mice with no detectable signal in control lung tissue images acquired under the same conditions. b, BAL cells of OVA-challenged mice show a predominance of eosinophils taking up and activating ProSense 680, with few eosinophils and little or no detectable fluorescence in BAL cells from control mice.

Imaging the dose response to dexamethasone: OVA-immunized mice received dexamethasone treatment (0.03, 0.3, and 3 mg/kg p.o.) administered before each intranasal challenge with OVA. Agent injection and tomographic imaging was performed as described under Materials and Methods. a, FMT imaging shows the sensitivity of optical tomography to detect and represent dose-dependent fluorescence differences in representative treated and untreated animals, with the highest dose of steroid reducing the fluorescence signal within the lung region to nearly the level seen in nondiseased control mice. b, ex vivo FRI of excised lung tissue confirms the dose-dependent effects on inflammation-related lung fluorescence and further reveals changes in the macroscopic distribution of the fluorescence with dexamethasone dose. Images are of representative mice within each group (n = 4/group), and the treatment study is representative of three treatment experiments.
Discussion
Noninvasive imaging techniques, both preclinically and clinically, are quickly becoming important tools in biomedical research leading to significant advances in a variety of disease areas, including osteoporosis, cancer, and cardiovascular disease. In particular, the potential of optical imaging has grown dramatically with the increased interest in biological readouts, rather than anatomical readouts, and the possibility of alternatives to the use of radioactive ligands for imaging. Recent breakthroughs in photonic technology have allowed the advance of optical imaging beyond standard, low-penetration two-dimensional FRI to allow for three-dimensional fluorescent tomographic in vivo imaging systems. Such technology has opened the door not only to deep-tissue detection and localization but also to the new capability of absolute quantification of fluorescence at any site within the body. Although imaging of preclinical mouse models of asthma has not been pursued extensively to date, the ability to use fluorescent imaging agents that detect and quantify a variety of biological activities has the potential to expand the horizons of asthma research and drug development.

Quantifying the dose response to dexamethasone. a, tomographic data sets of the treated and untreated OVA-challenged mice and control mice from the experiment represented in Fig. 5 were analyzed to quantify lung region fluorescence due to ProSense 680 activation. Dose-dependent decreases in total lung fluorescence (picomoles) and the volume of the fluorescence (millimeters cubed) were readily quantified in comparison to the signal measured in untreated OVA-challenged mice, with dexamethasone treatment showing less effect on the apparent affected lung volume than on the absolute magnitude of the inflammation. b, BAL cell analysis showed a predominant eosinophil influx in OVA-challenged mice, with the two highest doses achieving near-maximal inhibition of eosinophil cell numbers. c, noninvasive FMT quantification of ProSense 680 signal correlated well with BAL eosinophil counts. Ex vivo FRI of excised lung tissue confirmed the dose-dependent effects on inflammation-related lung fluorescence and also correlated well (r2 = 0.98) with FMT imaging (data not shown). Data represents the mean ± S.E.M. of all mice within each group (n = 4/group), and the treatment study is representative of four experiments. ANOVA analysis yielded statistical significance for the study (fluorescence, p = 0.001; BAL eosinophils, p = 0.0001), with asterisks indicating statistical significance by post-test analysis (*, p < 0.05; **, p < 0.01).
Pulmonary eosinophils are known to produce a variety of proteases, including secreted matrix metalloproteases, such as MMP-9, and -12, and lysosomal cysteine proteases, including cathepsins B, L, and S (Zheng et al., 2000; Cimerman et al., 2001; Lanone et al., 2002; Fulkerson et al., 2006). Such proteases are believed to play important roles in asthma pathogenesis, either directly in the degrading of extracellular matrix and airway remodeling or in basic inflammatory cell function. In a recent study (Cortez-Retamozo et al., 2008), researchers successfully used specific near-infrared sensors of protease activity to tomographically image and quantify disease severity in a murine model of asthma by focusing on extracellular MMP activity (predominantly MMP-12). MMPs are clearly important in asthma pathogenesis and a powerful approach for studying asthma pathogenesis; however, assessing cathepsin activity could provide more specific quantification of pulmonary eosinophilia for two reasons; 1) cathepsins are intracellular (allowing for specific cell internalization of imaging agents), whereas MMPs are predominantly secreted to the extracellular environment; and 2) MMPs play additional eosinophilic roles in asthma pathogenesis, complicating interpretation of noninvasive imaging results. Our studies successfully demonstrated the utility of quantitative fluorescence tomography (the FMT 2500 in vivo imaging system), paired with a cathepsin-activatable imaging agent (ProSense 680) to quickly, noninvasively, and accurately measure the severity of pulmonary eosinophilia in mice. OVA-challenged mice showed high levels of significant and consistent lung region fluorescence, whereas healthy control mice showed approximately 10-fold less lung signal. We further established that the eosinophil is the predominant cell type in the lungs of OVA-challenged mice that internalizes and activates a cathepsin-activatable agent, thus yielding a fluorescent signal that provides a biomarker for eosinophilia.
Inhibition of pulmonary eosinophilia using therapeutic doses of the steroid dexamethasone caused an accompanying decrease (up to 79%) in the amount of fluorescence quantified tomographically within the lungs. In contrast, imaging with an MMP-activatable agent showed a trend of ∼30% decreased lung signal, with no statistical significance but an 80% decrease in BAL eosinophilia (Cortez-Retamozo et al., 2008). Our quantified decrease in lung fluorescence with ProSense was dexamethasone dose-dependent, with maximal inhibition of eosinophilia seen using 0.3 to 3.0 mg/kg doses of this steroid. Careful dissection and imaging of lung tissue using FRI techniques confirmed the presence of significant fluorescence within OVA-challenged lungs and the airway localization of the signal, and this tissue signal correlated with the quantitative tomography. In addition, the quantitative imaging results with ProSense 680 correlated extremely well with established metrics for mouse asthma, such as BAL eosinophilia and histologic characterization of disease, with the fundamental difference being that the quantitative tomography is performed in live mice, whereas the established metrics require terminal procedures and animal death.
Although BAL cell counts have been shown to correlate well with pathology assessed by histological means, FMT imaging offers a powerful technique whereby the entire infiltrate (tissue and BAL) can be assessed simultaneously in a noninvasive fashion. Relatively few mice are needed (n = 3–4/group) to detect 50% decreases in pulmonary inflammation, and power analyses (using our historical data to predict variability of differently sized groups) suggest that as few as nine to 10 mice/group would be required to detect statistically significant changes in groups with as little as 30% inhibition of disease. We also have refined and improved our analysis techniques for FMT imaging to provide a measure of the relative volume of lung tissue affected by the disease process, a measure not used in previous optical tomographic lung inflammation studies (Cortez-Retamozo et al., 2008; Haller et al., 2008). Basal volumes of fluorescence seen with ProSense 680 in normal lung are low when thresholded to minimize basal fluorescence from resident alveolar macrophages, whereas this fluorescence volume achieves >350 mm3 in diseased mice. As expected, this volume measure is less sensitive to treatment because it equally weights all intensity fluorescence above the analysis threshold; however, such analysis provides a measure of the volume of lung affected by residual inflammation (45% or more) even after successful treatment that achieves >90% decrease in eosinophil influx. It remains to be determined whether additional time is required after treatment to clear the residual, low-grade inflammation, allowing complete alignment of changes in total fluorescence and fluorescence volume assessment.
Our findings show that quantification of cathepsin-activated ProSense 680 signal provides a clear, noninvasive measure of pulmonary eosinophilia. In our assessment of ProSense 680 in quantifying disease severity, we report an excellent correlation to BAL eosinophilia (r2 = 0.97). In addition, dexamethasone treatment of OVA-challenged mice showed that the inhibitory effects on cathepsin activity corresponded very well to decreases in eosinophilia (79 and 93% inhibition, respectively). Future studies will improve on our cross-validation of fluorescence signal with histology and fluorescence-activated cell sorting to better understand the identity and function of those cells that activate ProSense 680 and remain in the lungs even after high-dose steroid treatment. We also will investigate the potential of multiplexing agents to simultaneously quantify vascular leak (pulmonary edema), MMP activity (eosinophilia and tissue remodeling), and cathepsin activity (eosinophilia) to provide a clearer understanding of the biological spectrum of disease pathogenesis in mouse pulmonary inflammation. Cross-validation of quantitative tomography with pulmonary lung function will also provide valuable comparisons that will fully explore the utility and sensitivity of this imaging technology.
In conclusion, we have demonstrated the ability of the FMT imaging to noninvasively visualize and quantify inflammation in the lung in a robust and consistent manner. The consistency of the quantitative tomography and its excellent correlation with BAL assessment of eosinophilia provide a powerful tool for quantifying the therapeutic efficacy of dexamethasone treatment both as absolute fluorescence and as the relative volume of affected lung. FMT imaging in asthma research, using new and existing fluorescent imaging agents, will provide useful, noninvasive tools for understanding pulmonary inflammation and to help develop new therapeutics.
Acknowledgments
We thank Dr. Ralph Weissleder, Dr. Mikael Pittet, and Dr. Virna Cortez-Retamozo (Massachusetts General Hospital Center for Molecular Imaging Research, Boston, MA) for guidance in establishing asthma imaging protocols.
Footnotes
-
This work was supported by VisEn Medical, Inc.
-
Parts of this work were presented previously: Korideck H and Peterson JD (2008) Noninvasive quantitative tomography of disease progression and therapeutic response in a mouse model of asthma in vivo. World Molecular Imaging Congress 2008; 9–13 Sep 2008; Nice, France. Society for Molecular Imaging, Kerrville, TX.
-
Article, publication date, and citation information can be found at http://jpet.aspetjournals.org.
-
doi:10.1124/jpet.108.147579.
-
ABBREVIATIONS: FRI, fluorescence reflectance imaging; FMT, fluorescence molecular tomography; NIR, near infrared; MMP, matrix metalloprotease; BAL, bronchoalveolar lavage; OVA, ovalbumin; PBS, phosphate-buffered saline.
- Received October 24, 2008.
- Accepted March 16, 2009.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}