Article Text

Abstract
Background: Children who survive very low birth weight (VLBW) without major disability have a high prevalence of learning difficulty, attention deficit, and dyspraxia.
Aims: To determine whether learning difficulty in children with VLBW is associated with structural brain abnormalities.
Methods: A total of 87 children (aged 15–16 years) with a history of VLBW (<1500 g) and eight age matched full term controls have been studied with detailed magnetic resonance brain scans. Volume measurements of the caudate nuclei and hippocampal formations were made.
Results: Scans in 42.5% of the children showed evidence of perinatal brain injury. There was no significant difference in IQ, dyspraxia, or attention deficit between children with qualitatively normal and abnormal scans. However, quantitative volumetric analysis showed that children with a low IQ had smaller volume measurements for the right caudate nucleus and left hippocampus, and a smaller hippocampal ratio (left volume:right volume) than those with normal IQ.
Conclusion: Data suggest that learning disorder, attention deficit, and dyspraxia in children who survive VLBW do not correlate with conventional markers of perinatal brain injury, and may be related to global brain growth and the development of key structures, such as the caudate nuclei and hippocampal formations.
- very low birth weight
- learning difficulty
- MRI
- brain
- ADHD, attention deficit hyperactivity disorder
- CAPA, child and adolescent psychiatric assessment
- CSF, cerebrospinal fluid
- MRI, magnetic resonance imaging
- VLBW, very low birth weight
Statistics from Altmetric.com
- ADHD, attention deficit hyperactivity disorder
- CAPA, child and adolescent psychiatric assessment
- CSF, cerebrospinal fluid
- MRI, magnetic resonance imaging
- VLBW, very low birth weight
In recent years the survival of very preterm infants has improved greatly, stimulating an increased interest in their later neurodevelopmental progress. Despite major morbidity in 10–15% of very low birthweight (VLBW) survivors (<1500 g) the great majority enter mainstream school.1,2 Further studies of these children during their early school years have shown that 30–40% experience learning difficulties, behavioural problems, or dyspraxia.3,4 Although these problems may improve with time, most tend to persist in some form into adolescence.5,6 The aetiology of this loose syndrome of difficulties has variously been attributed to early cerebral injury, poor brain growth, maturational delay, socioenvironmental causes, or an interaction of two or more of these.
Magnetic resonance imaging (MRI) defines cerebral anatomy with a precision not previously available and with minimal invasiveness, making it an ideal investigational research tool in childhood neurodevelopmental problems. While most early MRI studies concentrated on structural lesions and defects in myelination which were associated with cerebral palsy and visual defects, more minor neurodevelopmental sequelae have also been studied.7,8 Minor cerebral infarcts in children with sickle cell disease correlated well with minor motor impairment detected by the Movement ABC.9 Differences in the size of the corpus callosum,10 and in the volumes of the caudate nuclei and the hippocampus have been observed in children with attention deficit or learning disorders who were born at term.11–17 The caudate nuclei receive inputs from cortical regions implicated in executive functioning and attentional tasks. Their relative size within the brain, and between right and left nuclei alters with maturation,18 although this process may be interupted by a variety of insults. The hippocampus is involved among other functions in learning and memory, and is also vulnerable to changes in volume associated with stress and other insults.
MRI volumetric assessments would seem to be a promising tool for the investigation of a variety of neurodevelopmental and behavioural disorders in children. The findings to date have been inconsistent and not easily replicable, possibly because of small studies, and variations caused by technique, gender, handedness, and body size.19
This study was designed to test the hypothesis that low intelligence, attention deficits, and dyspraxia in children at school who were born very preterm were related to evidence for abnormal development of the caudate nuclei and hippocampus on MRI.
METHODS
A cohort of 137 VLBW infants attending mainstream schools was studied in detail up to the age of 13 years. They had been followed up prospectively from birth, with formal examinations at school at 6 and 13 years, together with age and sex matched full term classroom controls. They have undergone detailed assessment of educational attainment, intelligence, attention span, motor skills, and visual acuity.3,5,6 IQ was measured using the Wechsler Intelligence Scale for Children III, and motor disability was assessed using the Movement ABC. Learning difficulties were assessed using the Suffolk Reading Scale, the Basic Mathematics Test, and the SPAR spelling test. Attention deficit hyperactivity disorder (ADHD) was assessed by Rutter A and B questionnaires with Connor’s Hyperactivity Scale, completed by parents and teachers. Psychiatric assessments were also performed for anxiety, fears, depression, antisocial behaviour, and self esteem. A child and adolescent psychiatric assessment (CAPA) interview was conducted with the child and parent.20 Visual function studies of acuity, steriopsis, and contrast sensitivity were also done. All of these data have been previously reported in detail , and only the IQ scores, Movement ABC scores, and the presence of attention deficit at 13 years were used in this study. For the purposes of this study low IQ was taken as being less than 85, and dyspraxia as a score on the Movement ABC at or below the 5th centile (total score of 13.5 or above). Children with Movement ABC scores between the 5th and 15th centiles were considered to have borderline impairment and were not considered to have dyspraxia for the purpose of this study.
Those children living within an hour’s journey from Liverpool were invited by letter to attend for an MRI scan. Full explanations of the purpose and nature of the study were given. The children were aged 15–17 years at the time of the scan. They were not paid for participating, but expenses were met in full.
Magnetic resonance scans were performed on a Philips Gyroscan NT5 scanner with a field strength of 0.5 Tesla (Philips Medical Systems, Best, Netherlands). A T1 weighted 3D (volume) gradient echo sequence (TR = 200 ms, TE = 30 ms, TI = 13 ms, flip angle = 30 degrees) was used to produce a coronal acquisition with a slice thickness of 2 mm and a 1 mm overlap. From this sequence, caudate and hippocampal volumes were measured on a Gyroview workstation (Philips Medical Systems, Best, Netherlands).
Scans were reported as showing evidence of thinning of the corpus callosum, lateral ventricular enlargement, periventricular leucomalacia, porencephally, or none of these. Measurements were made of the overall length of the corpus callosum, the cross sectional areas of the sagittal, left, and right transverse and coronal sections of the brain, the cross sectional area of the corpus callosum (entire and in thirds), and the coronal mid cross sectional areas of the right and left caudate nuclei. The cross sectional area of the corpus callosum as a percentage of the sagittal sectional area of the brain, and the transverse and axial areas of the right and left caudate nuclei as a percentage of the transverse and axial sectional areas of the respective cerebral hemispheres, were also calculated.
Hippocampal volumes were measured using the technique previously described by Jack and colleagues.21,22 The anterior and posterior boundaries were defined, including the whole of the head of the hippocampus anteriorly and using the crus of the fornix as the posterior anatomical landmark. The in-plane boundaries were then traced sequentially on each slice. The head of the hippocampus was separated from the amygdala by the uncal recess of the temporal horn of the lateral ventricle; in cases in which the uncal recess was not patent, an arbitrary horizontal line was drawn through the most superomedial portion of the temporal horn. The boundaries of the hippocampal body and tail were defined laterally by cerebrospinal fluid (CSF) in the temporal horn of the lateral ventricle, superiorly by CSF in the choroid fissure, medially by CSF in the uncal and ambient cistern, and inferiorly by the interface between the grey matter of the subiculum and the white matter of the parahippocampal gyrus (fig 1). These anatomical landmarks have been shown to define reliably 90–95% of the total hippocampal volume.23
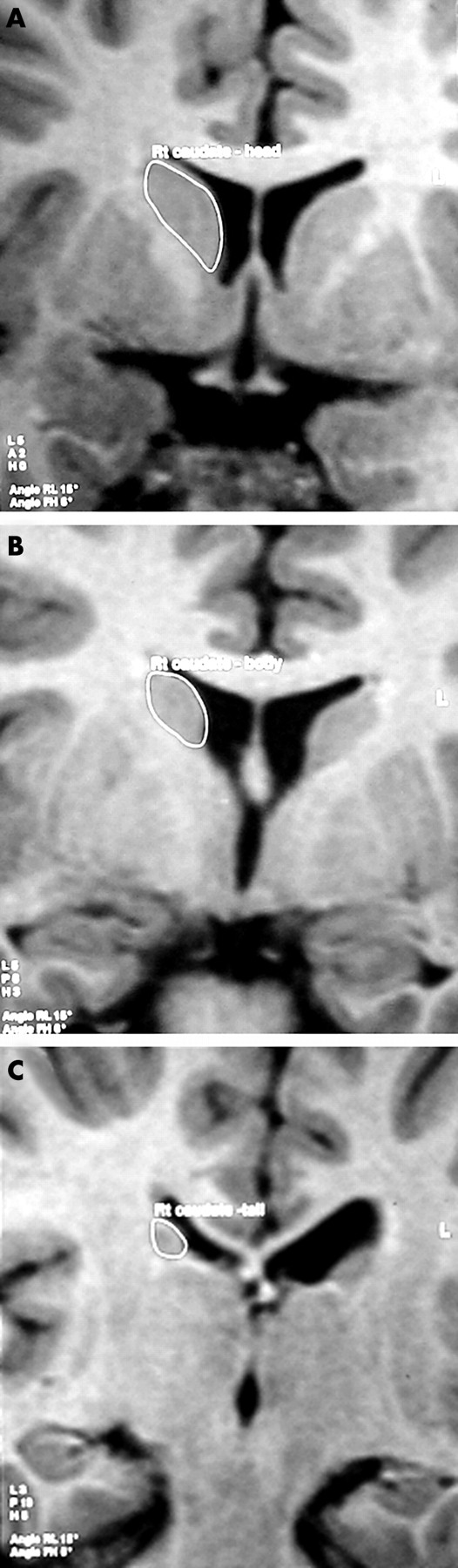
Coronal MR images showing the in-plane boundaries of the hippocampal formation: (A) head, (B) body, (C) posterior boundary at the level of the crus of the fornix.
Volumes of the caudate nuclei were measured using a similar technique. The boundaries of the caudate nucleus were defined anteriorly and laterally by the interface with the white matter of the frontal lobe and the anterior limb of the internal capsule, and medially by CSF in the lateral ventricle (fig 2). The posterior boundary was arbitrarily defined by the most anterior coronal section to show the crus of the fornix, as used to define the posterior boundary of the hippocampus. The slender tail of the caudate nucleus, which extends around the posterior part of the lateral ventricle, was not measured.

Coronal MR images showing the in-plane boundaries of the caudate nucleus: (A) head, (B) body, (C) tail.
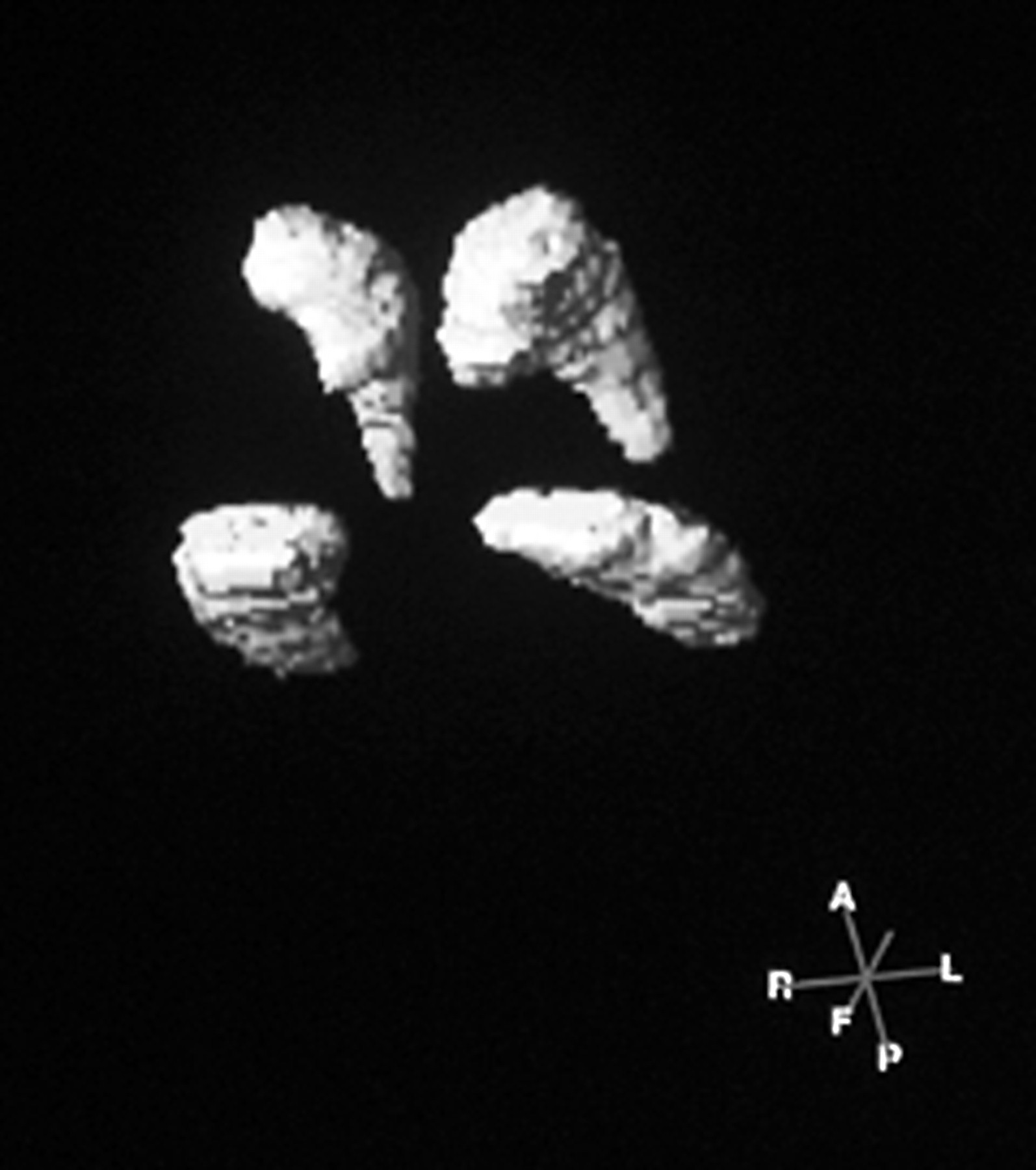
Once boundaries have been drawn on each coronal image, volumes were calculated automatically by the workstation using a volume of interest function. Surface rendered 3-D images were also generated as a check on anatomical accuracy (fig 3). The ratio of the volumes of the structures (left:right) was calculated as a percentage.
{kind=link}
{kind=link}
{kind=link}
Surface rendered 3-D reconstructions of the caudate nucleus and hippocampal formation generated from volume data on the Gyroview workstation.
Volume measurements were made independently by two observers (LJA and MP). Intraobserver and interobserver variation was calculated by the Bland–Altman method.24 For volume measurements of the hippocampal formations, 95% confidence limits of agreement (intraobserver) were between −161 and +165 mm3. For interobserver variation, 95% confidence limits of agreement were between −145 and +163 mm3. These results (less than ±7%) are comparable with those in previous studies,21 which have indicated that MR based measurements of these brain structures can be made with a high degree of reproducibility.
The study was approved by the Regional Paediatric Research Ethics Committee, and both child and parent gave written consent to the study.
RESULTS
Of the 110 children from the original cohort invited to take part, 96 replied and 87 were eventually scanned. Twenty six of the original controls were also approached and eight agreed to be scanned. The 87 index children had been born at a mean gestational age of 28.6 (1.7) weeks (range 24–35), and had a mean birth weight of 1103 (203) g (range 630–1500 g). All controls had been born at term. Nineteen children had been diagnosed as having ADHD, 30 as having a low IQ, and 33 as being dyspraxic.
The VLBW children had significantly smaller brains than controls on several measurements. Thirty seven (42.5%) of the index children had one or more abnormalities reported on their scans. None of the controls showed such abnormalities. No significant relation was seen between MRI scan appearances or linear and area measurements and ADHD, low IQ, or dyspraxia. These findings have been previously reported in detail.25
Table 1 shows the measurements of hippocampal and caudate volumes in VLBW subjects and controls born at full term. Caudate and hippocampal volumes were significantly higher in the term controls. Table 2 shows caudate and hippocampal volumes in subjects with ADHD and those without ADHD. Children with attention deficit had significantly smaller volumes of both right and left hippocampus.
Caudate and hippocampal volumes (mm3 (SD)) in controls and cases
Caudate and hippocampal volumes (mm3 (SD)) in cases with low IQ (<84) and higher IQ (>84)
Table 3 shows hippocampal and caudate volumes in subjects with low IQ (<85) and those with higher IQ (>85). Children with a low IQ had a significantly smaller right caudate nucleus and left hippocampus, and a lower hippocampal ratio when compared to those with a higher IQ.
Caudate and hippocampal volumes (mm3 (SD)) in cases with ADHD and cases without ADHD
No significant differences in caudate or hippocampal volumes were observed in children with dyspraxia when compared to those without.
Standardising for sex and handedness using logistic regression did not alter these findings.
DISCUSSION
This study has shown significant differences in volumetric measurements of the caudate nuclei and the hippocampus in adolescents born preterm and with attention deficit or low IQ when compared with “normal” preterm peers. No differences between those subjects with or without dyspraxia were observed. The caudate nuclei, but not the hippocampus, were significantly larger in term controls than in those born preterm. The hippocampal ratio (L/R×100) was significantly greater in term controls than in preterm subjects.
Hynd et al, in an early study of ADHD subjects, showed that the left caudate was significantly more often larger than the right in controls than in ADHD subjects.12 Castellanos et al showed a loss of right caudate dominance, because of a smaller right caudate, and suggested that age related changes in dominance had not occurred.14 In this study a significantly smaller right caudate was only seen in those preterm with lower IQ. Mataro et al more recently described a larger right caudate, and Filipek et al a smaller left caudate in ADHD subjects which appears to be the reverse of earlier findings.16,17
The hippocampus has been shown to be smaller in Alzheimer’s disease, temporal lobe epilepsy, complex febrile seizures, and post-traumatic stress disorder.26,27 In this study a smaller left hippocampus, and hippocampal ratio was seen in preterms with low IQ. In ADHD both right and left hippocampal formations appeared smaller and the ratio remained unchanged. A recent study of regional brain volume abnormalities and long term cognitive outcome in 25 preterm children at the age of 8 years by Peterson and colleagues28 has also shown that preterm children have smaller hippocampal formations and basal ganglia; in this study there is also evidence of an association with cognitive impairment.
As with previous reports of caudate size and asymmetry, there is considerable inconsistency in reported findings of the hippocampal size and ratios. The reasons for this have recently been reviewed.19 Gender, handedness, body size, developmental stage, and imaging variables all contribute to this variability. A recent paper by Obenaus and colleagues29 has described a standardised method for measurement and normalisation of hippocampal volume measurement in children of different ages; in our study, we were not able to perform this type of analysis, but all of the particpants in our study were 15–16 years of age, and the measurements in control subjects were similar to those previously found in adult studies. Standardising for gender and handedness in this study using logistic regression did not alter the findings.
Abnormalities in brain structure on MRI do not necessarily imply current aetiological significance, and may result from early environmental and genetic influences or physical insults. In particular, poor early postnatal growth, at a time of near maximal brain growth velocity, may be important in this regard. Poor performance in this cohort was associated with small stature and smaller head circumferences.30 Stress in older individuals may cause changes in growth of the hippocampus, possibly through the effect of high catecholamine concentrations on brain growth.27 Studies of cortical surface area and cortical convolution index in preterm infants who had grown poorly, showed reduced development at term compared with infants born at term.31 Greater attention to nutritional and environmental requirements of these infants in the newborn period might reduce the impact of premature birth on later learning and behavioural problems.
Acknowledgments
This study was funded by the Medical Research Council (grant number G9615155). We thank Mrs G Hughes, Mrs D Garlick, Mrs J Glynn, and Mrs H Tyrer for their skill and patience in performing the MRI scans, and the parents and children who gave their time to help in this study.
REFERENCES
Linked Articles
- Miscellaneous