


Abstract
The selective β3-adrenoceptor agonist mirabegron, an established alternative to antimuscarinic therapy for patients with overactive bladder, induces additional effects against receptors, transporters, and hepatic enzymes. The present study aimed to elucidate the effects of mirabegron on muscarinic receptors in the rat bladder using radioligand binding and functional assays. Mirabegron (0.1–100 μM) inhibited specific [N-methyl-3H]scopolamine methyl chloride binding in the bladder and other tissues of rats in a concentration-dependent manner. Binding affinity in the bladder was similar to that in the heart and significantly higher than those in the submaxillary gland and brain. Mirabegron induced the concentration-dependent relaxation of carbachol-induced contractions in the rat isolated bladder. Further analyses using a two-site model revealed that the relative quantities of high- and low-affinity components for mirabegron were 44.5% and 55.5%, respectively. Respective pEC50 values were 7.06 and 4.97. Based on the receptor binding affinity and pharmacokinetics of mirabegron, muscarinic receptor occupancy in the human bladder for 24 hours after the administration of a single oral dose of 50 mg mirabegron was 37%–76%. The present results demonstrate for the first time that mirabegron may relax the detrusor smooth muscle not only by β3-adrenoceptor activation but also muscarinic receptor blockade.
SIGNIFICANCE STATEMENT Mirabegron, the first selective β3-adrenoceptor agonist, represents an alternative to antimuscarinic agents for management of overactive bladder (OAB). The present study aimed to clarify whether mirabegron directly binds to muscarinic receptors and affects cholinergic agonist–induced contractions in rat urinary bladder and to predict muscarinic receptor occupancy in human bladder after oral administration of mirabegron. The results demonstrated that mirabegron therapy for patients with OAB may be due not only to β3-adrenoceptor activation but also muscarinic receptor blockade.
Introduction
Mirabegron (Fig. 1) is the first selective β3-adrenoceptor agonist to be developed for the treatment of patients with overactive bladder syndrome (Takasu et al., 2007; Chapple et al., 2014; Yamaguchi et al., 2019). It induces the β3-adrenoceptor–mediated relaxation of the detrusor smooth muscle in humans and rodents (Takasu et al., 2007; Svalø et al., 2013; Michel and Korstanje, 2016). Therefore, it may be administered instead of antimuscarinic agents to manage overactive bladder (OAB), for which antimuscarinics were found to be unsuitable because of adverse effects, including dry mouth, constipation, somnolence, drowsiness, and blurred vision (Deeks, 2018; Yamada et al., 2018). The off-target effects of mirabegron and its metabolites may be useful in therapeutic strategies for OAB (Dehvari et al., 2018). This agent has been shown to induce adverse effects against a number of related receptors, transporters, and hepatic enzymes (Takusagawa et al., 2012a,b; Alexandre et al., 2016; Mo et al., 2017; Groen-Wijnberg et al., 2017; Dehvari et al., 2018). With the exception of the effects of mirabegron on cardiac β1-adrenoceptors (Mo et al., 2017), which limit its administration to patients with heart conditions, the clinical significance of its off-target effects has not yet been elucidated.

Chemical structure of mirabegron.
Mirabegron has been shown to decrease acetylcholine release from cholinergic nerves in the urinary bladder of both rats and humans (D’ Agostino et al., 2015; Silva et al., 2017). Moreover, previous findings indicated that mirabegron antagonized muscarinic receptors in the bladder (Dehvari et al., 2018), however, the underlying mechanisms currently remain unclear. In material submitted to the Food and Drug Administration by Astellas Co., Ltd., mirabegron was shown to exhibit binding affinity to human M2 muscarinic receptors (Ki value of 2.1 μM) [U.S. Food and Drug Administration. Pharmacology/Toxicology NDA/BLA Review and Evaluation (NDA 202-611) 2012 (Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/202611Orig1s000PharmR.pdf)]. The proposed effects of mirabegron on muscarinic receptors warrant further study because combination therapy has been conducted for mirabegron with antimuscarinic drugs, such as solifenacin, which are established agents in first-line therapy for OAB (Herschorn et al., 2017; Gratzke et al., 2018; Kelleher et al., 2018). Combination therapy with solifenacin plus mirabegron has been associated with a higher incidence of anticholinergic adverse effects, such as dry mouth, than solifenacin alone (Herschorn et al., 2017; Kelleher et al., 2018). Therefore, the present study aimed to clarify whether mirabegron binds to muscarinic receptors and affects cholinergic agonist–induced contractions in the urinary bladder by using a radioligand binding assay of muscarinic receptors in the rat bladder and other tissues as well as a functional assay with isolated bladder strips. Muscarinic receptor occupancy in the human bladder and submaxillary gland after the oral administration of mirabegron at a clinical dose was estimated based on receptor binding affinity and pharmacokinetic parameters.
Materials and Methods
Materials.
[N-Methyl-3H]scopolamine methyl chloride ([3H]NMS) (3.03 TBq/mmol), a radioligand that selectively binds to muscarinic receptors, was purchased from PerkinElmer Life Sciences, Inc. (Boston, MA). Mirabegron and other chemicals were obtained from commercial sources.
Animals.
Eight-to ten-week-old male Sprague-Dawley rats, which were used to measure urodynamic parameters and receptor binding, and 12- to 14-week-old female Wistar rats, which were used to assess contractile responses in isolated bladders, were purchased from Japan SLC, Inc. (Shizuoka, Japan). Rats were housed in the laboratory with free access to food and water and maintained on a 12-hour light/dark cycle in a room with a controlled temperature (23 ± 1°C) and humidity (55% ± 5%). Experimental protocols received approval from the Committee for Research at the University of Shizuoka and Mukogawa Women’s University and were performed in accordance with the guidelines for the care and use of laboratory animals of both universities.
Measurements of Muscarinic Receptor Binding Activities in Tissues.
Muscarinic receptor binding activities were measured in the bladder and other tissues of rats using a radioligand binding assay with [3H]N-methylscopolamine as a selective radioligand, as previously described (Oki et al., 2005; Maruyama et al., 2006). The bladder, submaxillary gland, heart, and brain (cerebral cortex) were dissected, washed with cold saline, and minced with scissors. Tissue was homogenized with a Kinematica Polytron homogenizer in 19 volumes of ice-cold 30 mM Na+/HEPES buffer (pH 7.5). The homogenate obtained was centrifuged at 40,000g at 4°C for 20 minutes. The resulting pellet was resuspended in the same buffer as that for the binding assay. The radioligand binding assay for muscarinic receptors was conducted using [3H]NMS. In the binding assay, tissue homogenates were incubated with [3H]NMS (0.10–0.30 nM) in 30 mM Na+/HEPES buffer (pH 7.5) (assay volume: 1 ml) at 25°C for 60 minutes. Rapid filtration (cell harvester; Brandel Co., Gaithersburg, MD) through Whatman glass microfiber B grade (GF/B) filters terminated the reaction, and the filters were rinsed with 3 ml of ice-cold buffer three times. Tissue-bound radioactivity was then extracted from the filters by immersion in scintillation fluid overnight, and radioactivity was assessed using a liquid scintillation counter. Specific [3H]NMS binding was calculated experimentally as the difference in counts obtained in the absence (total binding) and presence (nonspecific binding) of 1 μM atropine. The fraction of total binding relative to the amount of radioligand per tube was 0.12–0.20.
Measurement of Contractile Responses in Isolated Bladder Strips.
The bladder was removed from each rat under sodium pentobarbital anesthesia (120 mg/kg, i.p.) and immediately placed in oxygenated Krebs’ solution (NaCl 118.4 mM, KCl 4.7 mM, CaCl2 2.5 mM, MgCl2 1.2 mM, NaHCO3 25 mM, NaH2PO4 1.2 mM, and glucose 11.1 mM) at 37°C. The upper part of the bladder was vertically divided into four parts. The middle third of the detrusor muscle was cut into bladder strips (2 mm wide × 5 mm long), which were mounted in a 10-ml organ bath containing Krebs’ solution at pH 7.4, maintained at 37°C, and continuously gassed with 95% O2/5% CO2. Isometric tension was recorded using a force-displacement transducer (model t-7; NEC San-Ei, Tokyo, Japan) coupled to a dual-channel chart recorder (model 8K21; NEC San-Ei). Strips were placed under a passive tension of 2.94 mN and then equilibrated for 45–60 minutes prior to the initiation of further experiments. The effects of mirabegron on carbachol (3 μM)-induced contractions by isolated rat bladder strips were then investigated. This agent was cumulatively applied to the organ bath after the stimulation with 3 μM carbachol. Data were calculated as a change in values with 100% as the contractile force at 3 μM carbachol in the absence of any agents. The effects of 5-hydroxymethyltolterodine (5-HMT), an antimuscarinic agent, and isoproterenol, a β-adrenoceptor agonist, on carbachol-induced bladder contractions were simultaneously examined as references.
Estimation of Muscarinic Receptor Occupancy by Mirabegron in the Human Bladder and Submaxillary Gland from Unbound Plasma and Urine Concentrations.
The muscarinic receptor occupancies of mirabegron in the bladder (RObladder) and submaxillary gland (ROs. gland) were estimated based on unbound concentrations in plasma (Cplasma,u) and urine (Curine,u) using the following equations: in which IC50 s. gland and IC50 bladder are IC50 for specific [3H]NMS binding in the rat bladder and submaxillary gland, respectively, assuming that the interstitial concentrations of mirabegron in the submaxillary gland and bladder may be approximated to Cplasma,u and urine Curine,u, respectively. Cplasma,u and Curine,u were calculated using the following equations:
in which IC50 s. gland and IC50 bladder are IC50 for specific [3H]NMS binding in the rat bladder and submaxillary gland, respectively, assuming that the interstitial concentrations of mirabegron in the submaxillary gland and bladder may be approximated to Cplasma,u and urine Curine,u, respectively. Cplasma,u and Curine,u were calculated using the following equations: in which Cplasma is the plasma concentration of mirabegron, fu is the unbound fraction of mirabegron in plasma, CLr is the renal clearance of mirabegron, and UP is the rate of urine production (liter per hour). Cplasma and CLr were obtained from a previous study by Krauwinkel et al. (2012) in which 50 mg mirabegron was orally administered to healthy elderly subjects. CLr, fu, and UP were 8.75 l/h (Krauwinkel et al., 2012), 0.29 (Dickinson et al., 2013), and 0.076 l/h (Yokoyama et al., 2013), respectively.
in which Cplasma is the plasma concentration of mirabegron, fu is the unbound fraction of mirabegron in plasma, CLr is the renal clearance of mirabegron, and UP is the rate of urine production (liter per hour). Cplasma and CLr were obtained from a previous study by Krauwinkel et al. (2012) in which 50 mg mirabegron was orally administered to healthy elderly subjects. CLr, fu, and UP were 8.75 l/h (Krauwinkel et al., 2012), 0.29 (Dickinson et al., 2013), and 0.076 l/h (Yokoyama et al., 2013), respectively.
Data Analysis.
The present study was exploratory in the sense of the editorial. Data are shown as mean ± S.D. Competition binding data obtained from experiments using rat tissue membranes were analyzed using the nonlinear regression analysis program GraphPad Prism (Version 7.0; GraphPad Software Inc., San Diego, CA) with a one-site binding model. Data from contractile responses in the isolated rat bladder were fit via nonlinear regression to monophasic or biphasic models using GraphPad Prism. In accordance with the exploratory nature of the present study, all P values within the manuscript cannot be interpreted as hypothesis testing, only as descriptive.
Results
Binding Activities of Mirabegron to Muscarinic Receptors in the Bladder and Other Tissues of Rats.
Mirabegron (0.1–100 μM) inhibited specific [3H]NMS binding in the bladder (Fig. 2A), submaxillary gland, heart, and brain (cerebral cortex) (Fig. 2B) of rats in a concentration-dependent manner. The pIC50 values of mirabegron for the inhibition of specific [3H]NMS binding were 5.62 ± 0.21 (bladder), 4.61 ± 0.26 (submaxillary gland), 5.69 ± 0.10 (heart), and 4.90 ± 0.09 (brain) (Table 1). The IC50 value of mirabegron in the bladder was similar to that in the heart and approximately 11- and 5-fold lower than those in the submaxillary gland and brain, respectively, indicating the higher affinity of this agent to muscarinic receptors in the bladder and heart than those in the submaxillary gland and brain. The Hill coefficient (slope factor) of mirabegron in each tissue was close to unity, except for in the bladder, in which it was less than one (Table 1).

Inhibition of specific [3H]NMS binding in rat tissues by mirabegron and 5-HMT [(A) bladder, (B) submaxillary gland (S.gland), heart, and brain]. Muscarinic receptors in rat tissues in the absence and presence of each agent at various concentrations were measured by a radioreceptor binding assay using [3H]NMS as the selective radioligand of muscarinic receptors. The ordinate was shown as percentage of the control-specific binding of [3H]NMS in the absence of any agents. Each point represents the mean ± S.D. of four (5-HMT) and five (mirabegron) measurements for the bladder (A) and four for each tissue (B). M: molar concentration.
pIC50 values and Hill slopes for the inhibition of specific [3H]NMS binding by mirabegron in the submaxillary gland, bladder, heart, and brain of rats
The antimuscarinic agent 5-HMT (0.3–30 nM) (Maruyama et al., 2006) induced the concentration-dependent inhibition of specific [3H]NMS binding in the rat bladder (Fig. 2A) with a pIC50 value and Hill coefficient of 8.19 ± 0.09 and 1.15 ± 0.60 (n = 4), respectively. The β-adrenoceptor–selective agonist isoproterenol (1–100 μM) did not markedly affect specific [3H]NMS binding in the rat bladder (unpublished data).
Relaxant Responses of Cholinergic Contractility in the Rat Bladder by Mirabegron.
As shown in Fig. 3A, mirabegron at concentrations of 0.1 nM–100 μM caused the concentration-dependent relaxation of carbachol (3 μM)-induced contractions in isolated rat-bladder smooth muscles, and the concentration-response curves of mirabegron were typically shallow. Relaxant responses at low concentrations (0.1 nM–1 μM) of mirabegron were followed by further relaxation at higher concentrations (1–100 μM). An analysis of biphasic relaxant curves using a biphasic model revealed that the relative quantities of high- and low-affinity components for mirabegron were 44.5% and 55.5%, respectively, whereas pEC50 values for these two components were 7.06 and 4.97 (Fig. 3B), respectively.
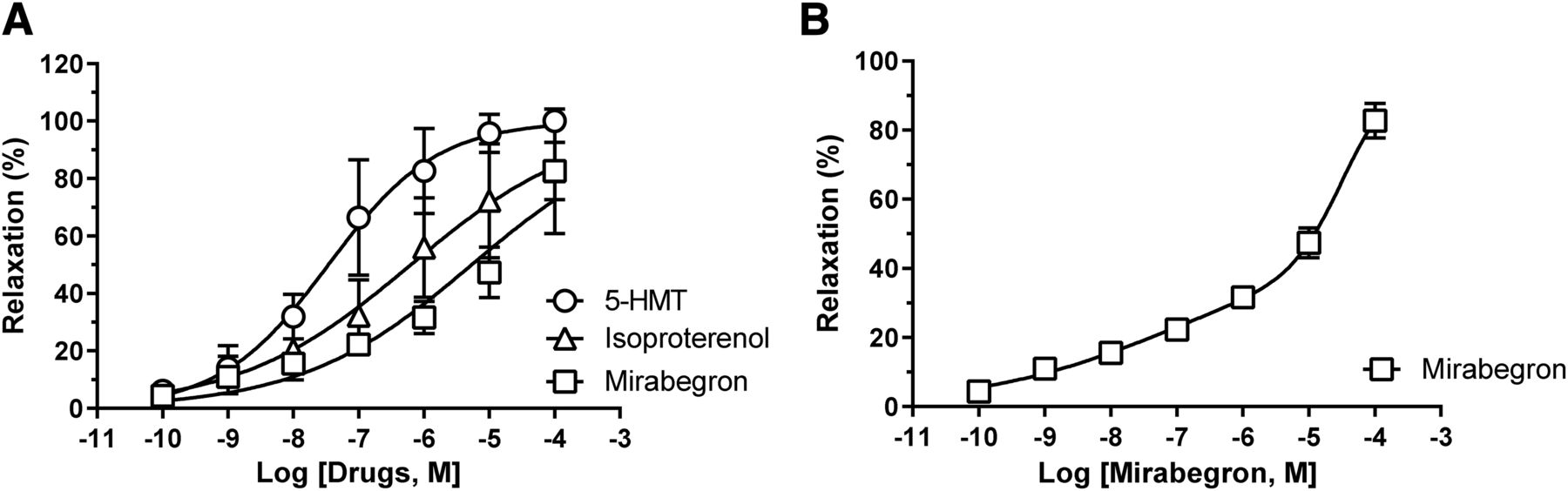
Inhibitory effects of mirabegron, 5-HMT, and isoproterenol at various concentrations on contractile responses in isolated rat-bladder strips induced by carbachol (3 μM). The concentration-dependent relaxation of carbachol (3 μM)-induced contractions in rat isolated bladder strips by each agent (A) was measured. The ordinate was shown as percentage of the control response of carbachol in the absence of any agents. Mirabegron-induced relaxation was further analyzed using a biphasic model (B). Each point represents the mean ± S.D. of six (5-HMT), three (isoproterenol), and five (mirabegron) measurements. M: molar concentration.
5-HMT (0.1 nM-100 μM) caused the concentration-dependent relaxation of carbachol (3 μM)-induced contractions in rat isolated-bladder smooth muscle with a pEC50 value of 7.50 (Fig. 3A). Similarly, isoproterenol (0.1 nM–100 μM) relaxed carbachol-induced contractions in a concentration-dependent manner, with a pIC50 value of 6.12.
Prediction of Muscarinic Receptor Occupancy in Human Tissues by Oral Mirabegron.
A previous study reported that the estimated unbound concentration of mirabegron in plasma reached approximately 20 nM 4 hours after the administration of a single oral dose of 50 mg mirabegron to healthy elderly subjects (Krauwinkel et al., 2012) (Fig. 4A). The CLr of mirabegron (8.75 l/h) was 5-fold higher than its glomerular filtration clearance (fu × glomerular filtration rate = 1.7 l/h), indicating that the urine concentration of mirabegron is concentrated in the renal tubules by the tubular secretion and reabsorption of water. Based on these pharmacokinetic parameters, the urine unbound concentration of mirabegron was estimated to be 1.6–8.2 μM, which was 400-fold higher than its plasma unbound concentration (Fig. 4A). Muscarinic receptor occupancy in the human bladder was estimated from muscarinic receptor binding affinity in the rat bladder and the pharmacokinetic binding parameters of oral mirabegron as described in the Materials and Methods. Predicted receptor occupancy was 37%–76% for 24 hours after the administration of a single oral dose of 50 mg of mirabegron, as shown in Fig. 4B. However, muscarinic receptor occupancy in the human submaxillary gland estimated from the unbound plasma concentration of mirabegron was less than 1%.

Estimation of the unbound concentration of mirabegron in plasma and urine (A) and muscarinic receptor occupancy in the bladder and submaxillary gland (S.gland) (B) after the administration of a single oral dose of mirabegron (50 mg) to healthy elderly subjects. Cplasma and CLr after the oral administration of 50 mg mirabegron to healthy elderly subjects were obtained from a previous study by Krauwinkel et al. (2012). CLr, fu, and UP were 8.75 (Krauwinkel et al., 2012), 0.29 (Dickinson et al., 2013), and 0.076 l/h (Yokoyama et al., 2013), respectively. The unbound concentration and muscarinic receptor occupancy of mirabegron were estimated using these pharmacokinetic parameters, as described in the Materials and Methods.
Discussion
β3-Adrenoceptor mRNA is predominantly expressed in the human detrusor muscle (Fujimura et al., 1999; Nomiya and Yamaguchi, 2003). The selective β3-adrenoceptor agonist mirabegron is an established alternative to antimuscarinic therapy for patients with OAB. The present study is the first to demonstrate the muscarinic receptor binding affinity of mirabegron in the bladder and other tissues of rats as well as its antagonistic effects on carbachol-induced contractions in the isolated bladder detrusor muscle.
Specific [3H]NMS binding in the bladder, submaxillary gland, heart, and cerebral cortex of rats was suppressed by mirabegron in a concentration-dependent manner. These results provide direct evidence for the first time of the binding of a β3-adrenoceptor agonist to muscarinic receptors in the bladder and other tissues. Five types of muscarinic receptors (M1-M5) have been identified to date, and the M2 and M3 subtypes were previously shown to be strongly expressed in the bladder detrusor muscle (Ito et al., 2009). The M3 receptor has been identified as the primary mediator of detrusor contractions in response to cholinergic activation (Yamanishi et al., 2015). M3 muscarinic receptors were found to be predominantly or exclusively expressed in the salivary gland, such as the submaxillary gland, whereas the M2 and M3 subtypes were both detected in the bladder, with a predominance of the M2 receptor (Wang et al., 1995; Ito et al., 2009; Yoshida et al., 2010). The M1 subtype is predominantly expressed in the cerebral cortex (Oki et al., 2005). The present results revealed that the IC50 values of mirabegron for specific [3H]NMS binding were significantly lower in M2 subtype–dominant bladder and heart than in the M3 subtype–dominant submaxillary gland or M1 subtype–dominant cerebral cortex (Table 1), which provides supportive evidence for the higher affinity of mirabegron for the M2 subtype than for the M3 and M1 subtypes.
Previous studies that investigated the mirabegron-mediated relaxation of the detrusor muscle in humans and rodents used muscle precontracted with carbachol, with pEC50 values of 6.54–5.29 for mirabegron (Takasu et al., 2007; Svalø et al., 2013; Cernecka et al., 2015; Michel and Korstanje, 2016). The EC50 value of mirabegron-induced relaxation in rat bladder strips precontracted with carbachol was 5.1 μM (Takasu et al., 2007). Similar EC50 values have been reported by other studies (Michel and Korstanje, 2016). Although mirabegron-mediated relaxation was detected in rat detrusor muscle precontracted with carbachol or KCl, this response appeared to be stronger in the former (Cernecka et al., 2015).
In the present study, mirabegron at concentrations of 0.1 nM–100 μM caused the concentration-dependent relaxation of carbachol-induced contractions in isolated rat bladder smooth muscles, and the concentration-response curve of mirabegron was shallow (Fig. 3A), which is consistent with previous findings (Takasu et al., 2007; Svalø et al., 2013; Cernecka et al., 2015; Michel and Korstanje, 2016; Dehvari et al., 2018). Cernecka et al. (2015) reported shallow concentration-dependent relaxant curves for mirabegron in the rat and human urinary bladders. Dehvari et al. (2018) obtained similar findings (Hill slope of less than 1) for mirabegron in the detrusor muscle of both humans and rodents in comparisons with isoprenaline-mediated relaxation. Collectively, the present results and previous findings indicate the presence of heterogeneous binding sites for mirabegron or negative cooperativity, suggesting binding to more than one site in the detrusor muscle. The relaxant response observed at low concentrations (0.1 nM–1 μM) of mirabegron appeared to be followed by further relaxation at higher concentrations (1–100 μM). The analysis using the biphasic model revealed that the relative quantities of high- and low-affinity components for mirabegron were 44.5% and 55.5%, respectively (Fig. 3B). Respective EC50 values were 87.3 nM (nanomolar range) and 10.7 μM (micromolar range). The efficacy for the low-affinity component of the relaxant response of carbachol-induced contractions to mirabegron in the rat bladder was consistent with its micromolar binding affinity to competitively inhibit specific [3H]NMS binding by muscarinic receptors in the rat bladder (Table 1). These results indicated the involvement of muscarinic receptors in the relaxation of bladder smooth muscle by relatively high concentrations of mirabegron. Therefore, the efficacy of mirabegron to relax the detrusor muscle may result from not only β3-adrenoceptor activation but also muscarinic receptor blockade.
The clinical significance of the effects of mirabegron on muscarinic receptors in the bladder was investigated in more detail. The pharmacokinetics of mirabegron and the clearance of tissue-bound mirabegron need to be considered. The maximal plasma level of mirabegron in elderly subjects after a single oral dose (50 mg/day) was approximately 85 nM (Krauwinkel et al., 2012). Furthermore, a previous study reported the rapid absorption of mirabegron after its administration to subjects at an oral dose of 50 mg per day for 7 days; time to reach maximum plasma drug concentration (Tmax) was 3 to 4 hours, the terminal plasma half-life was ∼60 hours, and ∼71% of mirabegron bound to plasma proteins (Krauwinkel et al., 2012). The administration of a single oral dose of [14C]mirabegron to rats was shown to elevate tissue:plasma radioactivity levels in some organs, with ratios increasing to 20 after its repeated administration, and it was then slowly eliminated from a number of tissues, including the kidney (Dehvari et al., 2018). Based on these pharmacokinetics, the concentration of mirabegron is assumed to be markedly higher in bladder tissue than in plasma because this agent may be concentrated by the tubular secretion and reabsorption of water in renal tubules. The results of the pharmacokinetic analysis indicated that the unbound concentration of mirabegron in the urine of elderly subjects after a single oral dose of 50 mg was approximately 2–8 μM at its maximum (Fig. 4A). Higher concentrations of mirabegron may be excreted in urine with a multiple-dose administration protocol (Krauwinkel et al., 2012). According to predictions by pharmacokinetics and micromolar receptor binding affinity, muscarinic receptor occupancy was estimated to be 37%–76% in the bladders of elderly subjects who received a single dose of 50 mg (Fig. 4B). Therefore, in the human bladder, mirabegron excreted in the urine appears to directly attenuate muscarinic receptor-mediated function, possibly by simple diffusion across the urothelium during urine storage.
Receptor occupancy was estimated based on two assumptions. One assumption is that the muscarinic receptor binding affinity of mirabegron in the bladder is similar in rats and humans. Mirabegron has been shown to have affinity for human M2 muscarinic receptors with a Ki value of 2.1 μM (http://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/202611Orig1s000PharmR.pdf). The affinity of mirabegron was similar in the rat bladder in the present study, with an IC50 value of 2.62 μM. In addition, solifenacin bound to muscarinic receptors in rat and human bladders with similar Ki values of 56 and 44 nM, respectively (Yoshida et al., 2014; Ito et al., 2016). These findings suggest that species differences in muscarinic receptor binding affinity in the bladder between rats and humans are small. Another assumption is that the interstitial concentration of mirabegron in bladder smooth muscle may be close to its urine concentration. In the bladders of mice subjected to bilateral ureteric ligation, total radioactivity (73%) and specific [3H]imidafenacin binding (63%) were markedly decreased by an intravenous injection of the radioligand to mice (Ito et al., 2017). These findings indicate that the majority of the radioligand in the bladder was supplied by the urine. Difficulties are associated with measuring interstitial drug concentrations in bladder smooth muscle. When interstitial concentrations of mirabegron were 0.5- and 0.2-fold that of the urinary concentration, muscarinic receptor occupancy in the bladder was estimated to be 23%–61% and 11%–39%, respectively (unpublished data). Mirabegron is considered to induce pharmacologically relevant muscarinic receptor occupation in the bladder; however, precise estimations of receptor occupancy based on interstitial concentrations are currently limited.
According to the findings of a systematic review and network meta-analysis by Kelleher et al. (2018), combination therapy with solifenacin (5 mg) and mirabegron (25 or 50 mg) was more effective than mirabegron (50 mg) alone but was associated with a higher incidence of anticholinergic adverse effects (dry mouth, constipation, and blurred vision) than solifenacin alone. Herschorn et al. (2017) also reported that the incidence of dry mouth, constipation, and dyspepsia was higher with combination therapy with mirabegron and solifenacin than with monotherapies. Therefore, the higher incidence of anticholinergic adverse events with combination therapy with mirabegron and solifenacin may be attributed to the antagonistic effects of mirabegron on muscarinic receptors in addition to β3 agonistic properties. The present results obtained using the rat bladder support the clinical relevance of the blockade of muscarinic receptors by mirabegron.
Authorship Contributions
Participated in research design: Yamada.
Conducted experiments: Chimoto, Shiho, Morikawa, Wakuda.
Performed data analysis: Okura, Wakuda, Shinozuka.
Wrote or contributed to the writing of the manuscript: Yamada, Okura, Shinozuka.
Footnotes
- Received August 25, 2020.
- Accepted February 12, 2021.
This work received no external funding.
The authors indicated no conflicts of interest.
Abbreviations
- CLr
- renal clearance
- fu
- unbound fraction of mirabegron in plasma
- 5-HMT
- 5-hydroxymethyltolterodine
- [3H]NMS
- [N-methyl-3H]scopolamine methyl chloride
- OAB
- overactive bladder
- UP
- rate of urine production pEC50 -log[50% effective concentration:EC50] pIC50 -log[50% inhibitory concentration:IC50]
- Copyright © 2021 by The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}