


Abstract
Sodium thiosulfate (STS) provides protection against carboplatin-induced ototoxicity in an animal model. The purpose of this study was to determine the STS dose required for otoprotection, in patients with malignant brain tumors treated with carboplatin in conjunction with osmotic blood-brain barrier disruption. Twenty-nine patients received STS intravenously 2 hr after carboplatin. Doses were escalated from 4 g/m2 to 8, 12, 16 and 20 g/m2on consecutive months. Audiologic assessment was performed at baseline and monthly. The audiograms were compared with those of 19 similarly treated historical control patients who did not receive STS. The incidence of ototoxicity in the historical control group of patients was 79% (15/19). This group had an average loss of 20.8 ± 5.9 dB (n = 19) at 8 kHz after one treatment with carboplatin, whereas the STS treatment group lost only 3.7 ± 2 dB (n = 15) after one treatment. This difference was statistically significant as assessed by Student’s ttest (P < .05). Furthermore, patients in the STS treatment group with excellent base-line hearing showed little change in hearing thresholds at 8 kHz after the second treatment (8.0 ± 8.3 dB) (n = 5) compared with the historical control patients with excellent base-line hearing, (40.5 ± 8.6 dB) (n = 11). Our data support that doses of 16 or 20 g/m2 of STS decrease carboplatin-induced hearing loss without central nervous system entry. Clinical demonstration of an otoprotective effect with a two-compartment system to prevent drug-induced hearing loss, while preserving central nervous system cytotoxicity, has not been reported previously.
Carboplatin is a highly effective chemotherapeutic agent against small-cell lung cancer and head and neck cancers (Canetta et al., 1985;Kosmidis et al., 1994). Its effectiveness has been demonstrated when used in conjunction with osmotic BBBD for the treatment of malignant brain tumors (Williams et al., 1995;Neuwelt et al., 1994). Unfortunately, unexpected high-frequency hearing loss was noted in a large portion of patients undergoing this regimen (Williams et al., 1995). Multivariate analysis of patients who received carboplatin suggested that furosemide and BBBD via the vertebral artery might be factors contributing to carboplatin-induced ototoxicity (Williamset al., 1995). Despite eliminating furosemide from the drug regimen, hearing loss continues to occur, although to a lesser degree. Unless the problem of ototoxicity can be addressed sufficiently, further use of carboplatin with BBBD in the treatment of brain tumors will be limited. Preclinical and clinical studies are being conducted to identify a chemoprotective agent to reduce carboplatin-induced ototoxicity (Dorr, 1991).
Carboplatin displays less nephrotoxicity, neurotoxicity and ototoxicity than its analog, cisplatin (DiRe et al., 1990; Goel et al., 1989; Howell et al., 1982; Iwamoto et al., 1984; Pfeifle et al., 1985). There have been previous reports of potential chemoprotective agents against cisplatin toxicity, including amifostine (WR-2721) and glutathione (Plaxeet al. 1994; Shpall et al.,1994; Demchak et al, 1991). One chemoprotective agent that has been studied broadly to reduce the nephrotoxicity of cisplatin is STS (Na2S2O3) (Dorr, 1991; Goel et al., 1989; Elferink et al., 1986). STS is used clinically as an antidote for cyanide poisoning and nitroprusside overdose at a dose of 12.5 g given intravenously for 10 min (American Regent, product information, 1992). Medical contraindications for the administration of STS include sodium-retaining conditions such as cirrhosis of the liver, congestive heart failure and impaired renal function. Hypertension may be exacerbated. After intravenous injection, STS is distributed throughout the extracellular fluid, crosses the BBB poorly and is rapidly excreted unchanged in the urine, with a biologic half-life reported to be 0.65 hr (American Regent, product information, 1992). Indeed at 5 hr after a wide range of doses, Pollay and Kaplan (1971) reported STS levels of 5% and 10% of brain and cerebrospinal fluid levels, respectively.
STS prevents cisplatin cytotoxicity in vitro (Abe et al., 1986) and decreases cisplatin nephrotoxicity in animals (Iwamoto et al, 1984). Two-route chemotherapy, with the combination of intraperitoneal cisplatin with intravenous STS, has shown positive results in human cancers by decreasing cisplatin-induced nephrotoxicity (Goel et al., 1989; Howell et al, 1982; Pfeifle et al., 1985). The combination of intra-arterial cisplatin with intravenous STS has been effective in head and neck cancer, allowing for escalation of the cisplatin dose while decreasing nephrotoxicity (Robbins et al., 1996). Clinical demonstration of an otoprotective effect from an agent such as STS to prevent drug-induced hearing loss has not been reported.
Animal studies have demonstrated the chemoprotective activity of STS against carboplatin-induced ototoxicity (Neuwelt et al., 1996). In a guinea pig model, STS decreased carboplatin-induced ototoxicity, determined by electrophysiological measurements of auditory function and counts of remaining inner ear outer hair cells. In this model, protection occurred when STS was administered up to 8 hr after carboplatin but not 24 hr after carboplatin. In a rat model of osmotic BBBD, STS was neurotoxic (i.e., induced seizures) when given immediately after BBBD, but not when given 60 min after BBBD, when the barrier is re-established (Neuwelt et al., 1996). Current studies (unpublished data) indicate that STS is also otoprotective against cisplatin-induced hearing loss in the guinea pig.
STS and other reactive thiols are thought to act by direct binding and inactivation of platinum-containing DNA-alkylating agents such as cisplatin and carboplatin. Rapid covalent binding of the platinum drugs depends on a high concentration of STS (Elferink et al., 1986). A molar ratio of STS to cisplatin of 500 is necessary to block the antiproliferative activity of cisplatin in vitro (Abeet al., 1986). Previous in vitro studies demonstrated that 40-fold molar excess of STS completely blocked the cytotoxic effects of carboplatin (Neuwelt et al., 1996). STS is ideal for chemoprotection of nephrotoxicity because it is excreted rapidly by the kidneys and thus achieves the locally high concentration necessary for drug inactivation. The purpose of the current project was to determine the STS dose required for sufficient otoprotection after enhanced carboplatin delivery and to identify the toxicities associated with that dose. Carboplatin was administered intra-arterially in conjunction with osmotic opening of the BBB which in animal studies (unpublished data) increases delivery 16-fold, an increase that is consistent with other water-soluble markers (Neuweltet al., 1998). The STS was given intravenously after the BBB was reestablished, thus creating a two-route, two-compartment system (fig. 1).

Two-compartment model. (A) Delivery of carboplatin across the BBB. Carboplatin is administered immediately after osmotic shrinkage of the BBB with hypertonic mannitol. The chemotherapeutic agent is able to cross the opened BBB (Neuweltet al, 1996). (B) Exclusion of STS from the brain. STS is administered at 2 hr after BBB disruption, after the BBB permeability has returned to base-line levels. The highly charged STS molecule does not cross the BBB (Pollay and Kaplan, 1971).
Patients and Methods
The study was approved by the Institutional Review Board of the Oregon Health Sciences University, and informed consent was obtained from each patient (or the patient’s legal guardian) in accordance with institutional regulations. As patients entered the protocol they were required to undergo base-line audiologic assessment that included air and bone pure tone thresholds and word discrimination tests. Monthly audiograms were collected within 24 hr before the patient’s treatment with BBBD plus carboplatin chemotherapy. BBBD was performed with the patient under general anesthesia, as described previously (Neuweltet al., 1991; Neuwelt and Dahlborg, 1989). Depending on the location of the tumor, 25% mannitol was infused (5–10 ml/sec) into the appropriate carotid or vertebral artery for 30 sec. The combination chemotherapy regimen consisted of intravenous cyclophosphamide (330 mg/m2), beginning approximately 20 min before the mannitol infusion, followed immediately by intravenous etoposide (200 mg/m2). A 10-min intra-arterial infusion of carboplatin (200 mg/m2) was begun 5 min after the mannitol infusion. Patients generally underwent two infusions monthly on sequential days, and treatment with BBBD generally continued for up to 1 year.
Historical control group.
Between February 1992 and May 1995, 37 patients underwent BBBD with carboplatin treatment before the initiation of the STS trials. This historical cohort included patients with good base-line hearing as well as patients with significant base-line hearing loss unrelated to their chemotherapy. To accurately determine the effects of carboplatin on hearing, patients in this cohort who received furosemide, which is known to increase platinum ototoxicity, or patients who received ototoxic agents such as aminoglycoside antibiotics, were removed from the analysis, which left 14 patients in the cohort. In addition to these 14 patients, audiograms from five patients treated with carboplatin plus BBBD after May 1995, but before inception of the STS trial, are included in the control group. Thus the control group totaled 19 patients. Data regarding this group is shown in table 1.
Patient data for the historical “no STS” control group1-a
Figure 2A shows the decline in hearing in a representative patient in the historical control group after treatment with BBBD plus carboplatin-based chemotherapy. This audiogram is an example of the pronounced high-frequency hearing loss noted in the historical group. The decline in this patient’s hearing started early in the course of chemotherapy treatment, after only 2 months of BBBD with carboplatin; however, there was not a great deal of subsequent decline.

Effect of BBBD and carboplatin on hearing in historical control patients who did not receive STS. Patients were treated with the carboplatin chemotherapy regimen delivered with osmotic BBBD as described under “Patients and Methods.” (A) Patient audiogram. A series of audiograms from the right ear of a single representative patient were obtained before initiating brain tumor therapy (base line, 10/12/93) and at monthly intervals before the next treatment with BBBD and carboplatin (11/8/93, 12/8/93, 1/12/94, 2/9/94). Hearing thresholds determined at eight frequencies are expressed in decibels. The data from the left ear were the same. (B) Cumulative hearing loss. The change in hearing threshold, compared with the pretreatment base line, is shown for low frequencies (0.25, 0.5, 1 and 2 kHz) and for high frequencies (4 and 8 kHz). Data represent the mean change ± S.E.M. for the indicated number of patients.
The fact that numerous patients treated with the carboplatin regimen experienced a rapid, pronounced decline in hearing, particularly at high frequencies, formed the basis of this study. In the historical control group there was a large effect on hearing early in the course of carboplatin treatment, with 53% (10/19) of the patients suffering significant high-frequency hearing loss after only one carboplatin treatment. Within the group demonstrating ototoxicity, an average hearing threshold shift of 34.5 ± 7.3 dB was detected at 4 kHz and 43.5 ± 7.2 dB at 8 kHz after only one treatment period. In contrast to the audiogram of the single representative patient (fig.2A), hearing in the historical control group continued to deteriorate throughout the course of carboplatin treatment (fig. 2B). Although the progressive hearing loss in this group was more severe at 4 and 8 kHz, figure 2B illustrates the progressive change in auditory thresholds at low frequencies (0.25, 0.5, 1, 2 kHz) as well.
Route, timing and dose of STS treatment.
Between May 1995 and August 1997, STS was administered to patients undergoing BBBD in conjunction with carboplatin-based chemotherapy. STS was administered intravenously beginning 2 hr after administration of carboplatin when the BBB was reestablished. Initially, STS was administered as a 4 g/m2 intravenous bolus for 15 min, followed by a 6-hr slow intravenous infusion of 12 g/m2 only on the first day of BBBD treatment, as described for protection against cisplatin nephrotoxicity by Goel et al. (1989) and Markmanet al. (1985) and for nitroprusside toxicity (Ivankovichet al., 1983). After approximately 3 months, with no toxicity noted, STS was administered in conjunction with both sequential days of blood-brain barrier treatment. Heart rate, blood pressure, temperature, respirations and plasma and urine levels of STS were monitored. Based on pharmacokinetic studies the 6-hr slow infusion was eliminated, and the bolus dose was escalated to 8, 12, 16 and 20 g/m2, given intravenously for 15 min 2 hr after carboplatin. At least three patients received a dose at each level before any patient was escalated to the next level, with the exception of the 16 g/m2 dose (n = 2). With these doses, heart rate, blood pressure, temperature, respirations, arterial blood gases, serum electrolytes (sodium and potassium) and serum glucose were monitored at base line, immediately post bolus infusion of STS, and 15 and 30 min after infusion. Plasma and urine STS levels were obtained at the end of the infusion, and at 15 min and 24 hr thereafter.
STS assay.
STS was assayed in plasma, urine and cerebrospinal fluid by the methylene blue method described byIvankovich et al. (1983). Samples and standards were diluted with water for assay. To 5 ml of STS diluent containing 0.006 M KI, 0.17 M KBr and 0.007 M KH2PO4, 0.5 ml of sample or standard was added and stirred. To the mixture were added 5 drops of KBH4 (0.556 M in 0.2 M NaOH prepared daily) with stirring, 10 drops of acetone with stirring, 5 drops of 0.07 M Fe2(SO4)3in 2.6 M H2SO4 and 5 drops of N,N-dimethyl-p-phenylenediamine sulfate (1 g in 104 ml of 2.6 M H2SO4). The mixture was capped and vortexed for 30 sec, vented and vortexed for another 30 sec. The samples were allowed to stand for 10 min, and then absorbance was measured at 665 nm. The standard range of the assay was linear between 1 and 100 μg/ml with a correlation coefficient of 0.9961 (± 0.0028,n = 35).
Data analysis.
For the purpose of data analysis, patients in the historical control group were divided into two subgroups. One subgroup consisted of patients with borderline normal to impaired base-line hearing (impaired base-line hearing), and the other subgroup consisted of patients with good to excellent hearing (excellent baseline hearing). Impaired base-line hearing was defined as >20 dB HL at one frequency and/or >15 dB HL at two consecutive frequencies, within the range of 0.25 to 8 kHz. Excellent base-line hearing was defined as <20 dB HL at all frequencies within the range of 0.25 to 8 kHz. Patients in the STS treatment group also were subdivided into an impaired base-line hearing group and an excellent base-line hearing group with the same definitions as stated above. Patient audiogram results were analyzed with Excel software (Microsoft) and Deltagraph. In as much as this was a dose escalation study and the numbers in the treatment group decreased after each subsequent course of STS at a given dose, the decreasing “n” after up to four courses precluded the effective use of the standard analysis of variance. Accordingly, statistical significance was determined by Student’st test and was not corrected for multiple comparisons.
Results
STS pharmacokinetics.
The STS pharmacokinetic data from patients are shown in table 2. Plasma STS values increased in a linear fashion with increasing dose. At the highest dose (20 g/m2), plasma STS levels in patients were approximately 60% of levels observed in guinea pigs at a dose of 11 g/m2 (Neuwelt et al., 1996). As mentioned, BBBD plus chemotherapy is done routinely on 2 consecutive days. The mean plasma and urine STS levels obtained on day 2 were similar to those obtained on day 1 (data not shown). In two patients who were treated with the 4 g/m2 bolus infusion followed by a 6-hr slow infusion of 12 g/m2, cerebrospinal fluid levels at the end of the slow infusion were 7% (3.32 and 4.30 mg/dl) of the serum concentration of STS.
STS pharmacokinetics2-a
STS toxicity.
Twenty-nine patients received STS. The patients ranged in age from 2 to 68 years. Tumor types were primitive neuroectodermal tumor (n = 8), glioma (n = 12), metastatic cancer (n = 3), primary CNS lymphoma (n = 4) and germ cell tumor (n = 2). Of the 29 patients, 10 had no prior radiation or chemotherapy, 17 had prior chemotherapy and 10 had prior radiation.
At low doses of STS (4 and 8 g/m2) (n = 12), mild nausea and vomiting were noted in a few patients during the STS infusion. Thereafter patients were premedicated with 0.625 to 1.25 mg of droperidol. There were no changes in arterial blood gases at any dose. A mild increase in serum sodium was noted at 8 g/m2 and by 20 g/m2 the peak serum sodium had increased 10 to 15% above base line to 155 to 160 mEq/l (table 3). With high-dose STS (16 and 20 g/m2) (n = 17), the transient hypernatremia was associated in most patients with a transient increase in blood pressure (10–15%) that began midway through the 15-min infusion and lasted through the completion of the infusion. The transient increase in blood pressure began to resolve immediately after completion of the STS infusion. Premedication with an antiemetic was necessary to minimize nausea with high-dose STS.
Effect of STS on serum sodium3-a
Plasma glucose levels.
Immediately post infusion of STS doses of 8 and 12 g/m2, serum glucose levels were observed in the range of 40 to 60 mg/dl. Despite the measured hypoglycemia, patients showed no clinical signs of hypoglycemia. Initially, rapid screening for blood glucose in the recovery unit was performed with a bedside glucose monitor (One Touch II; LifeScan, Milpitas, CA), which uses reflectance spectrometry. In vitrolaboratory analysis revealed that when increasing doses of exogenous STS were added to patient blood, apparent glucose concentration was depressed significantly when this spectrophotometric assay was used, by as little as 10 μg/ml of STS. However, two alternate systems for measuring blood glucose used in the hospital clinical laboratory, the Boehringer Mannheim/Hitachi 747 Analyzer (Boehringer Mannheim Corp., Indianapolis, IN), which is an endpoint absorbance measurement for NADH production, and the Synchron CX System (Beckman Instruments, Brea, CA), which uses the reaction-rate glucose oxidase/O2electrode method, displayed no suppression of glucose activity by the presence of STS. Consequently, further monitoring of patients was performed only with these two instruments, and no change from normal glucose ranges was observed.
Efficacy of low-dose STS.
The initial group of patients to receive low-dose STS (4 or 8 g/m2) (n = 8) already had been treated with carboplatin-based chemotherapy; thus, STS was a later addition to this group’s treatment regimen. Once STS was added to their regimen, there was little change in average auditory thresholds. The observation that STS blocked progressive hearing loss was encouraging. Unfortunately, most of the treated patients had profound carboplatin-induced high-frequency hearing loss before beginning STS therapy with little additional hearing to be lost. This was apparent when the average change in threshold from base-line hearing before the initiation of STS in this group of patients was assessed.
We next began treating patients with low-dose STS from the beginning of their carboplatin-based treatment (n = 4). One of these patients was an infant and not evaluable. At low doses of STS, there was pronounced unilateral hearing loss (high-frequency greater than low-frequency) early in the treatment course. In addition, compared with the guinea pig model (Neuwelt et al., 1996), serum levels of STS were not as high as anticipated. At STS doses of 8 g/m2, the mean serum value immediately post bolus was 96.8 mg/dl. The lack of hearing protection afforded by 8 g/m2 of STS, in combination with the low serum levels achieved with this dose, suggested that higher doses of STS may be required for efficacy.
Efficacy of high-dose STS.
Figure3A illustrates base-line and monthly audiograms in a representative patient who received high-dose (16 and then 20 g/m2) STS from the first carboplatin-based treatment. There was little change in this patient’s hearing from base line during 2 months of the carboplatin regimen. These results, particularly when compared with the audiogram of the historical patient who did not receive STS (fig. 2A), were encouraging. High-dose STS apparently preserved hearing in this patient. High-dose STS was administered routinely thereafter to patients from the beginning of their carboplatin plus BBBD treatment. These patients are described in table 4 (n = 17). Of the 17 patients, two were not evaluable; one patient was unable to follow instructions, and one was treated with STS for 1 month but was too ill to undergo follow-up testing. Therefore, 15 patients remained in the analysis.
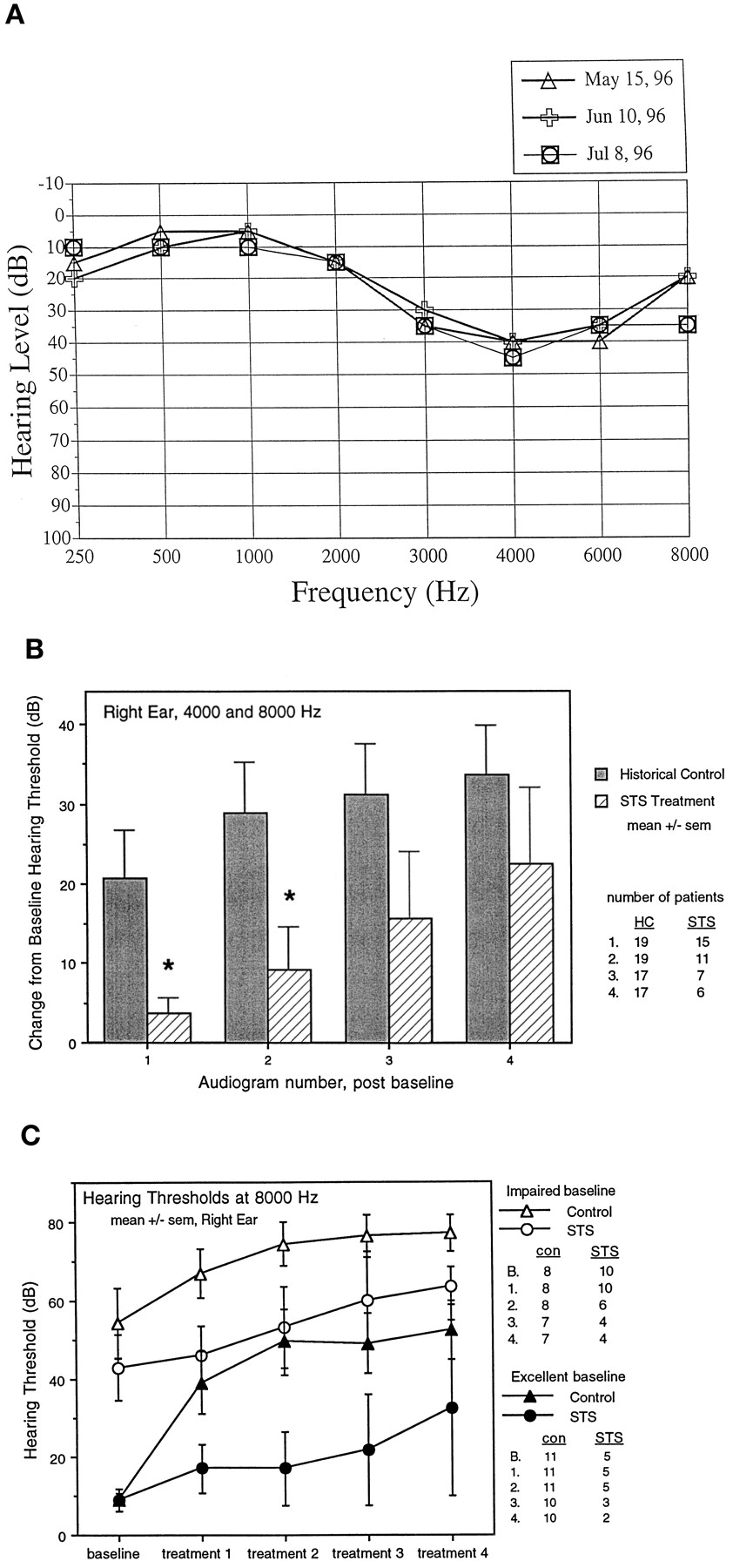
Efficacy of high-dose STS. These patients were entered into the STS protocol at high doses of STS (16–20 g/m2) and without previous exposure to BBBD and carboplatin. Patients were given STS 2 hr after monthly BBBD and carboplatin, as described under “Patients and Methods,” and monthly audiograms were performed. (A) Patient audiogram. A series of audiograms from the right ear of a single representative patient were obtained before initiating brain tumor therapy (5/15/96) and at monthly intervals before the next treatment with BBBD and carboplatin followed by STS (6/10/96, 7/8/96). Hearing thresholds determined at eight frequencies are expressed in decibels. The data from the left ear were the same. (B) Cumulative hearing loss. The change in hearing threshold, compared with the pretreatment base line, is shown for the historical control group (closed bars) and for the patients receiving high-dose STS (striped bars). Data represent the mean change ± S.E.M. in the threshold for the high frequencies (4 and 8 kHz) for the indicated number of patients (*P < .05). (C) Effect of STS on hearing thresholds at 8 kHz. The hearing thresholds (mean ± S.E.M.) are shown for the historical control patients (triangles) and the STS treatment patients who received 16 to 20 g/m2 STS (circles). Patients were assigned to excellent hearing and impaired hearing groups on the basis of their base-line audiogram, and monthly audiograms were performed. The number of patients is shown for each group at base line (B) and treatment with carboplatin and BBBD.
Patients treated with high-dose STS from the beginning of their BBBD plus carboplatin therapy4-a
Figure 3B illustrates the average change in hearing thresholds from base line in the 15 evaluable patients treated with STS for the first 4 months of carboplatin-based therapy, compared with the historical control group. This figure shows a distinct difference in auditory thresholds when the historical control group is compared with the high-dose STS treatment group, at frequencies of 4 and 8 kHz. When comparing the historical control group and the STS treatment group, without regard to base-line hearing, the historical control group suffered an average hearing threshold shift of 20.8 ± 5.9 dB (n = 19) after just one treatment with carboplatin, whereas the STS treatment group had a 3.7 ± 2 dB (n = 15) shift after one treatment. As assessed by Students’ t test, the STS treatment group had significantly less high-frequency hearing loss after 1 and 2 months of treatment than the historical control patients (P < .05). However, by 3 months of treatment (audiogram no. 3 post base line), the STS treatment group was no longer significantly better than the historical control because of the decreased number of patients at the later time points and their gradual increase in hearing loss. Serum STS levels at 16 and 20 g/m2 were 308 mg/dl and 330.8 mg/dl, respectively, immediately post bolus infusion (table 2). The STS data suggest that these levels of serum STS are not fully protective.
Of the 15 patients in the STS treatment group, 10 patients had borderline normal to impaired base-line hearing and five patients had excellent base-line hearing when using a definition of >20 dB HL at one frequency and/or >15 dB HL at two consecutive frequencies. When we analyzed the data by subgroup (patients with excellent base-line hearing and patients with impaired base-line hearing) data showed that patients with impaired base-line hearing were more likely to experience subsequent hearing loss than the patients with excellent base-line hearing. During the course of seven treatments, six patients (of 10) in the “impaired hearing” subgroup developed at least an additional 20-dB shift from base line, whereas two patients (of 5) in the “excellent hearing” subgroup suffered an additional 20-dB shift from base line. Given an ototoxicity rate of 20%, we would expect 2 of 10 patients to show ototoxicity. Because of statistical variation we may see more than this. The chances of more than 4 of 10 patients developing ototoxicity with a true ototoxicity rate of 20% is less than 5%. Thus at least 20% of patients with impaired base-line hearing demonstrate ototoxicity with a single dose of STS. Figure 3C shows hearing thresholds of the historical control group and patients treated with high-dose STS in the excellent base-line hearing and impaired base-line hearing subgroups, at 8 kHz.
Discussion
Dose and toxicity of STS in conjunction with BBBD.
Previous studies have shown positive results with the use of STS in conjunction with cisplatin, as a chemoprotectant against cisplatin nephrotoxicity (Goel et al., 1989; Howell et al., 1982; Pfeifleet al, 1985; Markman et al, 1985; Onoharaet al., 1988). However, the use of STS in humans as a potential protectant against either cisplatin- or carboplatin-inducedototoxicity has not been reported previously. Several studies report intravenous, bolus administration of STS at doses of 4 g/m2 followed by 12 g/m2infusion for 6 hr (Goel et al., 1989; Markman et al., 1985). Howell et al. (1982) reported a dose of 7.5 g/m2 given as an intravenous bolus followed by 2.13 g/m2 hourly by continuous infusion for 12 hr. Onohara et al. (1988) varied the dose of STS according to the amount of cisplatin being administered. Doses of STS in humans have not been reported as high as the 16 and 20 g/m2 dose we administered as an intravenous bolus for 15 min. In previous studies of STS as a chemoprotectant, no evidence of toxicity was reported (Goel et al., 1989; Howellet al., 1982; Pfeifle et al., 1985; Markmanet al., 1985; Onohara et al., 1988; Shea et al., 1984). In this study, transient hypernatremia occurred at a dose of 20 g/m2. Although patients tolerated the hypernatremia and had no associated clinical sequelae, there are no plans to administer a bolus dose greater than 20 g/m2. No signs of neurotoxicity were noted in the current patient population receiving STS 2 hr after BBBD. We have begun preliminary work investigating the administration of a second bolus dose of STS 6 hr after carboplatin. To date this regimen has been tolerated relatively well.
One potential concern is the possible reduction of carboplatin tumoricidal effect caused by inactivation of the chemotherapeutic drug by the chemoprotectant. We previously reported in vitrostudies which demonstrated that 40-fold molar excess of STS completely blocked the cytotoxic effects of carboplatin (Neuwelt et al., 1996). The blood-brain barrier essentially produces two compartments by limiting access to the brain. Carboplatin is administered in conjunction with BBBD, when the barrier is open. By 2 hr after BBBD the barrier is closed. At this point, the intravenous infusion of STS is administered. This delay in the STS administration provides a “partition” between carboplatin, which is administered while the barrier is open, and STS, which is administered after the barrier is closed. Administration of STS after a period of time sufficient for the transient alteration of the blood-brain barrier to return to base line should result in physical separation of the STS from the carboplatin delivered to tumor with BBBD, as shown schematically in figure 1. We hypothesize that because of this two-compartment approach, and because of the high ratio of thiosulfate/carboplatin necessary to inactivate carboplatin, it is unlikely that STS interferes with the cytotoxic effects of the CNS drug.
The potential that STS may inactivate systemic chemotherapy remains. A possible way to prevent a negative interaction could be to administer the STS at a later time after carboplatin. Our published studies in the guinea pig model show that STS is otoprotective even when administered 8 hr after carboplatin. Preliminary results from another guinea pig study suggest that a reduced dose of STS, achieving serum STS levels similar to a 16- to 20-g/m2 dose in humans, also will be protective at later time points. Our current preliminary clinical results, in which STS is administered 4 hr and 8 hr after carboplatin, are very promising. Maximizing the delay of STS administration may permit the use of STS after carboplatin or cisplatin for systemic (non-CNS) malignancies analogous to leukovorin rescue for methotrexate.
STS as an otoprotective agent.
Before the institution of STS, a high rate of carboplatin-induced ototoxicity was noted, especially at high frequencies. Once we began administering high-dose STS, we noted what appeared to be a preservation of hearing. Based on current data from patients with excellent base-line hearing, it appears that one 20 g/m2 dose of STS may provide hearing protection. Patients with excellent base-line hearing showed little change in hearing thresholds at high frequencies after either the first carboplatin treatment (mean loss = 8 ± 5.6 dB,n = 5, P < .05) compared with the historical control group with excellent base-line hearing [mean loss of 30.0 ± 8.4 dB (n = 11)], or the second treatment (8.0 ± 8.3 dB, n = 5) compared with 40.5 ± 8.6 dB (n = 11). In patients receiving 16 or 20 g/m2 of STS, serum STS levels approached 60% of the level known to be otoprotective in a guinea pig model (Neuweltet al., 1996). Our clinical impression is that in patients with excellent base-line hearing, although one bolus of high-dose STS apparently provides hearing protection, further patient accrual and analysis will be necessary to determine hearing efficacy.
In contrast, in patients with impaired base-line hearing, 50% of the patients developed at least an additional 20-dB threshold shift, although the loss was less then in the historical control patients. Therefore, it is clear that one 20 g/m2 dose of STS does not provide adequate protection in this group of patients. Because a single bolus dose of STS may be insufficient to prevent all chemotherapy-induced ototoxicity, we have begun a study of the efficacy of two boluses of STS in the guinea pig model of carboplatin-induced ototoxicity. One mechanism to increase the otoprotection provided by the maximum dose of STS may be to maintain plasma STS levels at a high level for an extended period.
Mechanism of carboplatin-STS chemoprotective reaction.
The precise mechanism for the chemoprotective reaction of STS against carboplatin is unknown. Elferink et al. (1986) investigated whether the basis of the reaction between STS and platinum complexes support a proposed “rescue” action by STS. When STS is administered with cisplatin, thus creating a high concentration of STS in kidney tissue, the reaction rate between cisplatin and STS is high, thus competition between thiosulfate and endogenous thiol groups for cisplatin may decrease renal tubular damage (Elferink et al., 1986).
We hypothesize that a reaction similar to that discussed by Elferinket al. (1986) occurs in the cochlea and is responsible for protection against ototoxicity. STS inactivates carboplatin in a manner similar to the inactivation of cisplatin in that the thiol binds the electrophil platinum, a complex that is excreted rapidly. The cochlea may act similarly to the kidney to concentrate STS in perilymph or endolymph. Thus high concentrations of STS in these compartments may inactivate carboplatin at the site of cochlear damage (Neuwelt et al., 1996) or it could have occurred in the plasma. Because only small volumes of endolymph and perilymph can be collected, we have been unable to test this hypothesis.
Additional potential chemoprotectants against chemotherapy-induced ototoxicity.
STS is not the only compound with otoprotective potential. Other clinically relevant compounds that may provide chemoprotection from carboplatin ototoxicity are glutathione andd-methionine. Increased glutathione levels decreased cisplatin-induced nephrotoxicity in preclinical (Anderson et al., 1990; Suzuki and Cherian, 1990; Zunino et al., 1989) and clinical (Gandara et al., 1991; Hamers et al., 1993) studies and also may decrease cisplatin-induced neurotoxicity (Cascinu et al., 1995; Hamers et al., 1993). Although a substantially increased dose of cisplatin was attainable when administered in conjunction with glutathione, cisplatin toxicity remained substantial and the number of tolerated chemotherapy cycles decreased (Plaxe et al., 1994).
In addition, Campbell et al. (1996) showed thatd-methionine, a sulfur-containing nucleophile that provides highly effective cisplatin nephroprotection, at a dose of 300 mg/kg administered 30 min before 16 mg/kg of cisplatin, provides complete otoprotection measured by auditory brainstem response and histology, in the rat. d-Methionine shows promise for use in humans, because parenteral d-methionine has been administered safely in humans for purposes such as radiographic imaging (Meyeret al., 1985). Future clinical trials in patients receiving platinum compounds may show benefits similar to the animal studies for the role of d-methionine as an otoprotectant in humans.
Platinum-based chemotherapy agents are very effective in the treatment of many cancers. The use of STS has broad implications for decreasing not only the nephrotoxicity of these agents but also the ototoxicity. The discovery of STS as an otoprotective agent allows for less toxicity associated with platinum-based chemotherapy, thus making these effective agents more tolerable to patients in the clinical setting and, when given in conjunction with our two-compartment model, allows further novel clinical trials of the platinum-containing cytotoxic agents.
Footnotes
-
Send reprint requests to: Edward A. Neuwelt, M.D., Oregon Health Sciences University, Blood-Brain Barrier Program, 3181 SW Sam Jackson Pk Rd - L603, Portland, OR 97201-3098.
-
↵1 This work was supported by the Veterans Administration Merit Review Grant and by National Institutes of Health grants RO1 CA31770 and NS33618.
- Abbreviations:
- Amifostine (WR-2721)
- BBBD
- blood-brain barrier disruption
- CNS, central nervous system
- HL
- hearing level
- STS
- sodium thiosulfate
- Received November 12, 1997.
- Accepted March 30, 1998.
- The American Society for Pharmacology and Experimental Therapeutics
References
JPET articles become freely available 12 months after publication, and remain freely available for 5 years.Non-open access articles that fall outside this five year window are available only to institutional subscribers and current ASPET members, or through the article purchase feature at the bottom of the page.
|




{kind=link}
{kind=link}
{kind=link}