Article Text

Abstract
Background—Carcinoid diarrhoea is associated with rapid small bowel and proximal colonic transit. Intravenous administration of a serotonin type 3 receptor (5HT3) antagonist restores postprandial colonic tone towards normal in carcinoid patients.
Aims—To evaluate the medium term effects of an oral 5HT3 antagonist, alosetron, on symptoms, stool fat, and transit in patients with carcinoid diarrhoea.
Methods—In 27 patients with carcinoid diarrhoea, symptoms were recorded daily and gastrointestinal transit was measured by scintigraphy in a three dose (0.1, 0.5, 2.0 mg, twice daily), randomised (1:1:1), parallel group, four week study. Placebo was given during the first week. Loperamide (2 mg capsules) was used as rescue medication.
Results—There were numerical improvements in median diarrhoea score, stool weight, loperamide use, and overall colonic transit at four hours, but no overall significant drug effect was shown. Alosetron reduced the proximal colon emptying rate (p<0.05 in 20 evaluable comparisons), but did not significantly alter small bowel transit.
Conclusions—Alosetron retardation of proximal colonic emptying in patients with carcinoid diarrhoea confirms the potential role of a 5HT3 mechanism in this disorder. Doses of alosetron higher than 2.0 mg twice daily will be required for symptomatic benefit in carcinoid diarrhoea.
- carcinoid diarrhoea
- alosetron
- serotoninergic agents
- antagonist
- colonic transit
Statistics from Altmetric.com
Carcinoid syndrome is a rare disease that affects approximately 600 patients per year in the United States. The two most common presentations of the carcinoid syndrome are diarrhoea and flushing, with the former occurring in approximately 80% of patients.1 ,2 The pathophysiology of carcinoid diarrhoea is incompletely understood, but there is a modest component of intestinal secretion,3 malabsorption of nutrients due to intestinal lymphangiectasia associated with mesenteric fibrosis,1 and motor dysfunction affecting the small intestine and colon.4 In a previous study, we have shown accelerated transit through the small intestine and colon, and a reduced capacitance of the ascending colon together with postprandial hypertonicity4; these are likely to contribute to the diarrhoea.
The putative mediators of carcinoid diarrhoea include substance P and serotonin,5 ,6 and previous work suggests that the serotonin type 3 receptor (5HT3) antagonist, ondansetron, is able to inhibit the postprandial tonic response of the colon in healthy individuals7 and to restore the hypertonic colonic response to a meal to normal levels in patients with carcinoid diarrhoea.8 These observations provide the basis for a clinical therapeutic study performed in patients with carcinoid diarrhoea. Four case reports have documented the reduction in stool frequency and increased stool consistency in a patient with carcinoid diarrhoea treated with the 5HT3 antagonists, ondansetron or tropisetron.9-12 Our general hypothesis, based on the normalisation of the colonic response of carcinoid patients by ondansetron,8 was that specific inhibition of 5HT3 receptors results in an improvement in the transit profile through the small intestine and colon, thereby facilitating reabsorption of luminal fluid, and ameliorating diarrhoea in these patients.
Alosetron (GR68755, molecular structure C17H18N4O.HCl) is a potent and selective 5HT3 receptor antagonist and is rapidly absorbed after oral administration. It is approximately five to 10 times as potent as ondansetron in vitro.13 In isolated tissue preparations, alosetron shows only weak activity at 5HT2receptors (pA2=5.2) and histamine H1 receptors (pA2=5.7), with a more than 5000-fold selectivity for 5HT3 receptors.13 It has no effect on 5HT1 or 5HT4 receptors. The bioavailability of alosetron in healthy volunteers is 60% and plasma half life is approximately 1.5 hours. Pharmacokinetics of single oral doses are linear up to 8 mg.13 Alosetron exhibited antiemetic effects in ferrets treated with cisplatin,14 but did not alter human stomach compliance or the perception of mechanical stimuli applied to the proximal stomach of healthy volunteers.15
In a preliminary report of a multicentre European and Canadian study, alosetron, 2 mg twice daily, was shown to reduce abdominal pain in patients with irritable bowel syndrome, particularly in those with loose or watery stools.16 Alosetron also increased colonic compliance and the distending volume required to elicit perception in patients with irritable bowel syndrome.17 Although there are no reports of effects of alosetron on gastrointestinal transit, it has previously been shown that ondansetron retards colonic transit in health and irritable bowel syndrome.18 ,19 We wished to expand on the acute experiments suggesting that 5HT3inhibition restores normal intestinal or colonic function8in patients with carcinoid diarrhoea. One approach to assess the principle indicated in our hypothesis is to perform a clinical trial. Thus, the aim of our present study was to assess the dose related, medium term effects of alosetron (0.1, 0.5, and 2.0 mg twice daily) on symptoms and gastrointestinal transit in patients with carcinoid diarrhoea.
Materials and methods
PATIENTS
Twenty seven patients with diarrhoea due to metastatic small bowel carcinoid syndrome were recruited for this study. One patient withdrew early, leaving 26 patients randomised to study medication. Their ages ranged from 37 to 81 years (median 67), and there were 16 men and 10 women. Patients were considered ineligible according to the following criteria: a maximum extent of small bowel or right colon resection exceeding 100 cm; or use of antibiotics, octreotide, or other antidiarrhoeal medications such as codeine, diphenoxylate, loperamide, or agents that alter gut transit (for example, calcium channel blockers, anticholinergic agents) within 48 hours of entry to the study. At baseline and at the end of the four week studies, patients underwent screening haematology, chemistry screens, and electrocardiography. Urinary 5-hydroxyindoleacetic acid (5HIAA) concentrations were measured to estimate tumour “load” prior to entry into the study. The study was approved by the Mayo Clinic Institutional Review Board, and all patients signed written informed consent.
EXPERIMENTAL DESIGN
Patients were entered into a three dose, randomised 1:1:1, parallel group, double blind study lasting four weeks. During the first week, all patients received the same placebo medication to obtain the baseline data for gastrointestinal transit as well as gastrointestinal symptoms. After four days, patients were contacted by the study coordinator to review symptoms and protocol instructions. After the first week, subjects were randomly assigned to receive alosetron 0.1, 0.5, or 2.0 mg, twice daily as two tablets with breakfast and dinner. For one day during the first and last week of the study, subjects underwent a gastric, small bowel, and colonic transit test over a period of 24 hours, and stool was collected during the transit evaluation in order to measure volume and fat content. During this 24 hour period, all meals were standardised: a 1.25 MJ breakfast meal consisting of egg (containing a radiolabelled marker), skimmed milk, and whole wheat bread; a 2.24 MJ chicken lunch ingested four hours after the radiolabelled breakfast; and a 2.36 MJ steak dinner ingested eight hours after the breakfast. Caffeine-free drinks were allowed throughout the 24 hour period. Cigarette smoking was not permitted throughout the transit tests. At the end of the four week study while on the study drug, patients returned for repeat bowel transit, stool weight, and stool fat measurements.
EFFICACY MEASURES
Symptom assessments
The two primary effectiveness measures were as follows:
A weekly self rating for diarrhoea using a 10 cm visual analogue scale which was unmarked and ranged from 0 (no diarrhoea) to 10 (the worst diarrhoea the patient had ever experienced). Patients also completed a daily diary for the entire four week trial period with categorical assessment of stool frequency, consistency, urgency, abdominal pain, number of “rescue” loperamide capsules used, and a daily self rated diarrhoea score. For analysis purposes, the baseline score was determined as the median of the seven daily scores (based on the raw data) measured during the first week during which all three groups received placebo. The scores from the 21 days of the active treatment trial were summarised as median weekly symptom scores for each subject. Improvement was defined by a change (20%) in average self rating during each of the final three weeks compared with the pretreatment rating. This cut off was used in view of the perception that this is the minimal improvement over placebo (or other available agents) that would render the novel medication a worthwhile addition to the therapeutic armamentarium. Dropouts were considered as “no improvement”. The physicians did not rate the patients’ symptoms in this study.
“Rescue”—Participants were given a supply of 2 mg loperamide capsules to be taken in a dose of two tablets (4 mg) up to four times per day: at 8 00 am, 12 00 noon, 6 00 pm, and at bedtime. Patients were instructed to avoid use of loperamide except when they developed severe diarrhoea and they or their primary physician were concerned that they were becoming dehydrated as a result. Moreover, subjects were instructed to take loperamide as rescue for only one day at a time and to continue experimental medication as required by the study. If the severe diarrhoea recurred during the night, the same course of action could be taken on a daily basis up to 15 times. The decision to use rescue was thus based on the severity of diarrhoea and risk of dehydration on each day of the study. If loperamide was used on more than 15 days, patients were deemed to be treatment failures.
In order to analyse the use of rescue medication, the time for use of five loperamide capsules, and the total number of loperamide capsules used were analysed as efficacy parameters, adjusting for the number of loperamide capsules used during the first week of single blinded, placebo treatment.
Transit profiles
The secondary effectiveness measures were the small bowel transit time, geometric centre of colonic radioisotopic count at four hours, and the proximal colon emptying rate.
Gastrointestinal transit, stool volume, and stool fat measurements
Gastrointestinal and colonic transit were measured scintigraphically using a delayed release, methacrylate coated capsule containing Indium-111 ion exchange pellets (Sigma Chemical, St Louis, Missouri, USA) for colonic transit and an egg meal (described earlier) containing Technetium-99m pellets (Sigma Chemical). These methods have been described in detail elsewhere20-23 including their use for estimation of the physiological efficacy parameters described earlier in carcinoid diarrhoea.4 Total stool weight, and fat and proportion of fat in stool were measured by a gravimetric method.24
DATA ANALYSIS
Primary effectiveness measures
Overall assessment of the diarrhoea was based on the median value of the daily visual analogue scale raw data for severity of diarrhoea during each week of the study. Loperamide rescue medication use (total number of capsules) and time to use five capsules were also determined from the daily diaries. Symptom improvement for each patient with complete data was also computed from average weekly diary scores (20% decrease in score versus week 1) for weeks 2, 3, and 4, and dropouts were considered as “no improvement”.
Secondary effectiveness parameters
The following transit data summaries acquired during weeks 1 and 4 were compared: small bowel transit time, colonic geometric centre at four and 24 hours, and proximal colonic emptying rate estimated from the instantaneous slope of the cumulative counts of isotope in ascending and transverse colon using an exponential model. Using the baseline values for transit as covariates, the three groups were compared to determine whether there was a drug effect.
Statistical analysis
The data values described earlier for each patient were analysed using an analysis of covariance (for example, weekly median diarrhoea scores) incorporating the corresponding values for the first week as the covariate. The time (number of days) to use five or more loperamide tablets was analysed using a proportional hazards regression analysis with initial week loperamide use (number of tablets) and treatment group (coded as dummy regression variables) as predictor variables. A one way, non-parametric analysis (Kruskal-Wallis test) was also used to compare treatment groups on the absolute changes (versus initial week) in data values. Finally, an extension of Fisher’s exact test was used to compare the proportions with improvement (no/yes = 20% decrease in scores) with dropouts considered as no improvement.
Results
CHARACTERISATION OF PATIENTS AND CARCINOID SYNDROME
Twenty seven patients with small intestinal carcinoid tumours metastatic to abdominal nodes or liver entered the study. One patient withdrew within one day of entry to the trial, but did not take any medication and was not considered further in the data analysis. One patient developed severe abdominal cramps and an “internal” flushing sensation, and withdrew on day 16 of the trial. One patient developed complications of carcinoid heart disease (heart failure) and had to be withdrawn from the trial on day 7, that is, the end of the placebo treatment week. Only one patient had intermittent symptoms consistent with partial small bowel obstruction prior to entry and did not develop obstruction during the study. Thus, 24 patients had evaluable data (of whom six in the highest dose group, eight in the mid and lower dose groups had complete baseline data). One patient developed metastatic ascites necessitating hospitalisation for ascitic fluid tap for symptom relief during the trial, but she completed the trial. In one patient who was blind, we were unable to obtain daily diaries of the patient’s symptoms or use of loperamide, and therefore only physiological parameters (transit and stool fat) were available for analysis. No other adverse effects were thought to be related to the study medication.
Table 1 summarises demographic data on the patient groups, stratified by randomisation to treatment dosage. There were no other significant adverse effects on haematology, biochemistry, or electrocardiography (data not shown). Note that, despite the blinded randomisation of groups, the group receiving the middle dose (0.5 mg twice daily) had somewhat lower urine 5HIAA and lower faecal fat than the group receiving the lowest dose of alosetron (0.1 mg twice daily). Baseline levels of diarrhoea scores were highest in the 0.1 mg dose group. Use of loperamide rescue was significantly (p=0.06) different among the three groups, with the 0.1 mg dose group using it most. To adjust for group dissimilarities, the baseline observations were used as covariates to assess the effects of treatment on clinical and physiological parameters during the three weeks of active treatment.
Demographics and characterisation of carcinoid diarrhoea at baseline
EFFECT OF ALOSETRON TREATMENT ON SYMPTOMS, STOOL FAT, AND WEIGHT
Table 2 shows the effects of the three doses of alosetron on symptoms, loperamide use, stool fat, and weight. The median weekly scores of individual symptoms, that is, frequency, consistency, urgency of bowel movements, and abdominal pain were not significantly altered by treatment (data not shown). Though the overall diarrhoea score appeared to change (table 2), this information was clearly influenced by the number of loperamide tablets used in each treatment group. The time to use at least five capsules of rescue medication (fig 1) and total rescue medication used were not significantly different after adjusting for baseline use of loperamide in the first week, though there appeared to be numerical differences in the use of rescue medicine in a dose related fashion (fig1).
Effect of alosetron on diarrhoea, loperamide use, stool weight, and stool fat on completion of the study

Cumulative use of rescue medication (loperamide) during the active treatment portion of the trial.
Alosetron did not significantly affect total stool weight, but the 0.5 and 2.0 mg doses produced a substantial reduction in mean stool weight (approximately 80 and 120 g per 24 hours respectively). Analysis of covariance failed to detect differences in the proportion of fat in stool among the three dose groups (p>0.1).
EFFECT OF ALOSETRON ON GASTROINTESTINAL AND COLONIC TRANSIT
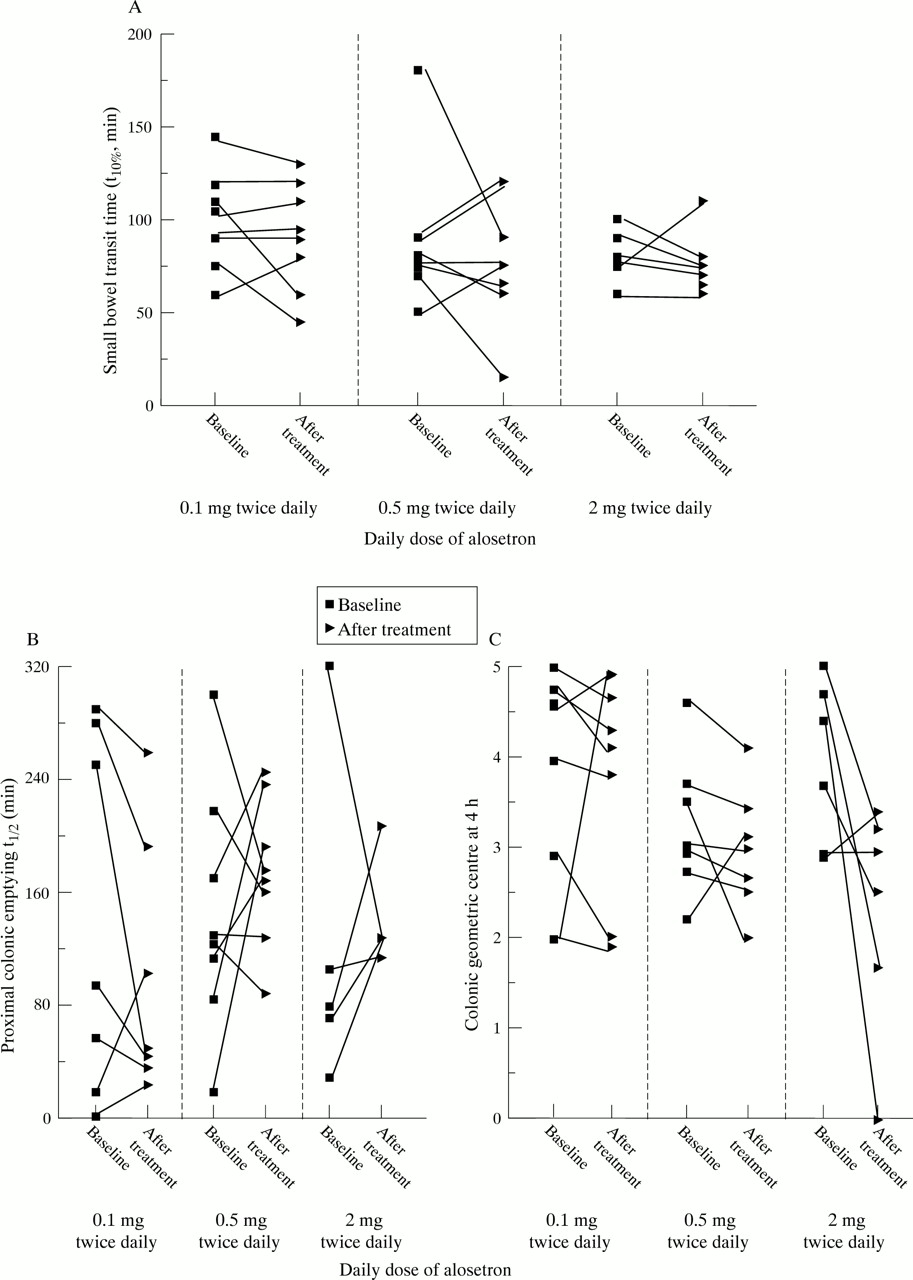
Alosetron did not affect gastric emptying or small bowel transit (fig 2A). The highest dose of alosetron appeared to change the value of the colonic geometric centre of isotope at four hours (fig 2B), but this was not statistically significant, in part due to variation among patients. Overall differences among groups were detected (p<0.05) in proximal colonic emptying, which was slower with the two highest alosetron doses (see table 3); this parameter was assessed in 20 of the 24 patients as technical reasons (for example, failure of capsule to empty from the stomach, failure of capsule dissolution) precluded this assessment in four patients. Figure 2B shows the t1/2 for proximal colonic emptying and fig 2C the colonic geometric centre at four hours. An increase in t1/2 indicates slower emptying post-treatment compared with baseline; a decrease in the colonic geometric centre at four hours post-treatment in three of the five patients treated with 2 mg alosetron indicates slower overall colonic transit since the weighted average of counts has a small numerical value.

{kind=link}
{kind=link}
Dose related effects of alosetron on small bowel transit time (A), proximal colonic emptying (t1/2) (B), and geometric centre at four hours (C) in patients with carcinoid diarrhoea.
Intestinal and colonic transit at baseline and after three weeks of treatment with alosetron
Discussion
With reference to the hypothesis that a 5HT3 mechanism is important in small bowel and colonic motility in carcinoid diarrhoea, our study has shown that the highest dose of alosetron used in this medium term trial significantly slowed proximal colonic emptying. This suggests that the 5HT3 effects may be localised to the proximal colon. There were also numerical, but statistically insignificant reductions in symptoms (median diarrhoea score), physiological parameters (stool weight), and a trend to reduced use of rescue medication. These three independent variables point in the direction of improvement in the clinical parameters assessed, but the doses used in this study were insufficient to show conclusively a beneficial effect on symptoms. It is conceivable that the relatively small sample size led to a type 2 statistical error.
The study provides several insights into the difficulties encountered in designing such therapeutic trials. Firstly, in an attempt to avoid the use of surrogate markers as primary efficacy objectives, we focused on the symptoms of stool frequency, urgency, and consistency. We performed a within study validation of our daily and weekly data collection and showed that there was a high level of congruence between the weekly overall assessment and a summary of the daily diaries averaged for each week of treatment. Secondly, the allowance of rescue medication for patients with severe diarrhoea introduced a confounding effect in the assessment of the symptoms. Moreover, use of rescue capsules of loperamide during the placebo treatment week (when patients were blinded to the nature of medication received) was significantly different among the three randomised groups. This was further confounded by the high correlation between use of loperamide during the placebo treatment period and the number of loperamide capsules used during the active treatment period. Our study, however, clearly indicates that even the highest dose was not effective in controlling symptoms despite the promising effects on proximal colonic emptying rate. Alosetron did not significantly alter stool fat or small bowel or overall colonic transit; however, the numerical trends in diarrhoea score, stool weight, and retardation of proximal colonic emptying are indicators that this form of therapy is promising and confirms the potential role of 5HT3 mechanisms in the development of carcinoid diarrhoea. Future studies will require higher doses or an alternative dosage schedule to assess clinical effectiveness.
A number of other confounding variables were encountered in this trial. For example, despite randomisation of patients, two factors were not equally balanced across groups: tumour secretion of serotonin (as assessed by urinary 24 hour 5HIAA excretion) and use of loperamide rescue in the baseline week. In a relatively rare disease such as carcinoid syndrome, with restrictive entry criteria for concomitant medications and extent of bowel resection (less than 100 cm), it is difficult to compensate for such confounding variables by expanding the sample population in a single centre. We chose a single centre strategy in this trial because of the need to perform repeated gastrointestinal and colonic transit measurements, which are not widely available. However, future studies with higher doses of alosetron should probably be performed in multiple centres, with focus on daily diaries for symptom evaluation.
At present, opioids and somatostatin analogues are the mainstays of symptomatic treatment in carcinoid diarrhoea.25 ,26Chemotherapy and interferons appear quite ineffective in symptom control or in reduction of tumour burden.26 ,27 Opioids alone are often ineffective clinically or are limited by their side effects. Octreotide requires subcutaneous injections three times daily and is generally very effective in symptom control of diarrhoea and flushing. Some patients require progressive increases in octreotide dose because of drug tolerance. With the higher doses of octreotide, there is a theoretical risk of inhibition of pancreatic exocrine and endocrine function28 with aggravation of diarrhoea or induction of fat malabsorption. However, this seems to be quite uncommon in clinical practice. Hence, somatostatin analogues are often the mainstay of treatment in carcinoid diarrhoea, and availability of efficacious oral analogues29 or depot parenteral preparations30 will be useful additions to the current therapeutic armamentarium.
Inhibition of the main mediators of carcinoid diarrhoea, such as serotonin and neurokinins6 has been a therapeutic approach for several decades, starting with the predominantly 5HT1antagonists, methysergide3 and cyprohep- tadine.31 We chose to attempt to antagonise the 5HT3 receptors because of recent work indicating their role in the control of colonic function in health,7 ,32irritable bowel syndrome,19 and carcinoid diarrhoea.8
This relatively large parallel group study of 24 evaluable patients with carcinoid diarrhoea has extended the experience previously reported in four single case studies of open treatment with 5HT3 antagonists in the literature.9-12 All the data published so far are consistent with the principle that serotoninergic type 3 antagonists may be effective in controlling carcinoid diarrhoea in the medium term. Moreover, we acknowledge that the present trial also suffers from the possibility of a type 2 statistical error in the evaluation of the effects of alosetron in view of the small sample size relative to the intrinsic variation in symptoms and transit parameters, as shown in the baseline studies.
In summary, in patients with carcinoid diarrhoea, alosetron significantly delayed emptying of the proximal colon, which in previous studies was shown to be the most abnormal physiological parameter in carcinoid diarrhoea.4 This was accompanied by a trend to a reduction in diarrhoea which, possibly due to the small sample size, did not achieve statistical significance; these effects were dose related. The results suggest that a 5HT3 mediated mechanism in the proximal colon is implicated in the pathophysiology of carcinoid diarrhoea and that inhibition of this mechanism may be important in treatment. Higher doses may be effective in inducing consistent clinical benefits.
Acknowledgments
This study was supported in part by the General Clinical Research Center grant no. RR00585 from the National Institutes of Health and by a grant from Glaxo Wellcome Research Foundation. We thank Mrs Carol Van Dyke for excellent technical support and Mrs Cindy Stanislav for typing and preparing this manuscript.