Article Text

Abstract
BACKGROUND The interaction between leucocytes and vascular endothelial cells is essential for leucocyte migration into inflammatory sites.
AIMS To study the local expression of the pairs of complementary molecules, α4β7/mucosal addressin cell adhesion molecule (MAdCAM-1) and OX40/OX40 ligand in the lamina propria of the colon and jejunum of patients with inflammatory bowel disease.
METHODS Ten patients with active ulcerative colitis (UC), nine with active Crohn's disease (CD), and seven irritable bowel syndrome (IBS) controls were submitted to endoscopic and peroral jejunal biopsies. Specimens were immunostained by indirect alkaline phosphatase using antibodies against CD3, intercellular adhesion molecule (ICAM) 1, α4β7, MAdCAM-1, and OX40. An OX40-mouse-IgG fusion protein was used to detect OX40 ligand on frozen sections. Immunohistological analysis was carried out by optical microscopy using a computer assisted image analyser.
RESULTS Colonic lamina propria of patients with CD and UC showed increased density of CD3+, α4β7+, and OX40+ cells compared with IBS controls. ICAM-1, MAdCAM-1, and OX40 ligand positive vessels were also increased compared with IBS controls. No significant difference was found in the density of any of these cells in the jejunal mucosa of patients compared with IBS controls.
CONCLUSIONS The expression of MAdCAM-1 and OX40 ligand on gut endothelial and OX40+ cells is increased in sites of mucosal inflammation in patients with inflammatory bowel disease. No evidence was found for increased lamina propria T cells or increased vascular adhesion molecule expression in the proximal intestine of patients with distal inflammatory bowel disease.
- adhesion molecules
- mucosal immunity
- T lymphocytes
- inflammatory bowel disease
Abbreviations used in this paper
- IBS
- irritable bowel syndrome
- IL
- interleukin
- TNF
- tumour necrosis factor
- ICAM
- intercellular adhesion molecule
- MAdCAM
- mucosal addressin cell adhesion molecule
Statistics from Altmetric.com
Inflammation is a complex response to localised stimuli, which comprises different immunologically competent cells and numerous mediator molecules. Vascular endothelial adhesion molecules and the synthesis and release of chemokines and cytokines have been implicated in the recruitment and emigration of inflammatory cells from the circulation to sites of inflammation. In the gut, increased endothelial cell expression of intercellular adhesion molecule (ICAM) 1, P-selectin, E-selectin, and mucosal addressin cell adhesion molecule (MAdCAM-1) has been observed in the inflamed colonic mucosa of patients with inflammatory bowel diseases.1-5 The increased expression of adhesion molecules on endothelial cells is mediated by proinflammatory cytokines such as interleukin (IL) 1 and tumour necrosis factor α (TNF-α)6-8 which are expressed at increased concentrations in the inflamed mucosa of patients with inflammatory bowel diseases.9-13
The interaction of the α4β7 integrin on a subset of T cells, with its ligand the mucosal vascular addressin MAdCAM-1, on endothelial cells has been shown to be responsible for the emigration of lymphocytes to inflamed sites in the gut.5 Increased expression of MAdCAM-1 on murine endothelial cells can be induced after stimulation with IL-1 and TNF-α.14 MAdCAM-1 has also been detected at high levels on islet vessels (high endothelial venule like vessels) in the pancreas of non-obese diabetic mice,15 on colonic lamina propria venules from mice with hapten induced colitis,16 or colitic IL-2 knockout mice.17 In another study using an animal model of colitis, the significant reduction in the number of lymphocytes in the colon ofscid mice reconstituted with CD45RBhigh CD4+ T cells after treatment with either a MAdCAM-1 specific antibody or a β7 specific antibody, suggests that this pair of molecules is clearly involved in cell traffic into inflamed gut.18
The human OX40 cell surface antigen is a glycoprotein expressed primarily on activated CD4+ T cells19 and it is a member of the TNF receptor family20 which plays important roles in growth, differentiation, and apoptosis of lymphocytes.21 The OX40 ligand (OX40L) is found on activated antigen presenting cells22 ,23 and the interaction with the OX40 receptor produces a potent costimulatory signal to CD4+ T cells.24 On the other hand, the recent demonstration of the constitutive expression of OX40L on human vascular endothelial cells suggests an additional role of the OX40/OX40L system concerning the trafficking and localisation of activated T cells.25 Given the specificity of OX40 for activated CD4+ T cells, and the strong evidence that Crohn's disease in particular is caused by an exaggerated CD4 Th1 response in the mucosa (reviewed in Pender and MacDonald26), it is of interest to determine whether OX40 is overexpressed in this condition.
Crohn's disease is often considered to affect the whole alimentary tract, although overt disease may be limited to a particular site.27 It is therefore important to determine whether the increased cellular infiltrate seen at distant sites reflects increased expression of vascular adhesion molecules, which in turn would reflect subclinical inflammation. In this work we have therefore studied the expression of α4β7 (Act-1) and MAdCAM-1 in Crohn's colitis as well as in the jejunum of the same patients. As controls we have also studied colonic and jejunal samples from patients with ulcerative colitis and irritable bowel syndrome. To extend these observations beyond MAdCAM-1/α4β7 interaction, which have been studied in inflamed tissue before, but not at distant sites, we have also investigated OX40/OX40L expression, which to our knowledge has not been analysed before in the gut.
Methods
PATIENTS
Jejunal and colonic biopsy specimens were taken from 10 patients with ulcerative colitis, nine patients with Crohn's disease, and seven patients with irritable bowel syndrome (IBS). The diagnosis of either ulcerative colitis or Crohn's disease was established by means of the usual clinical, radiological, endoscopic, and histological criteria.
The Crohn's disease group consisted of six women and three men with a mean age of 39.2 years (range 21–56). None of the patients had obvious jejunal involvement. In two of the patients the disease involved the ileum, in four the ileum and the colon, and in three the colon only. The disease had been present for a mean time of 5.2 years (range 1–13). At the time of biopsy, three patients were receiving only corticosteroids, two were receiving azathioprine, two were receiving corticosteroids and metronidazole, and three were not receiving any specific therapy. The two patients receiving azathioprine had distal fistulising disease and of the seven others, five had active mucosal inflammation and stenoses. According to the criteria established by Harvey and Bradshaw,28 all patients were in an active phase of the disease.
The ulcerative colitis group consisted of six women and four men with a mean age of 42.1 years (range 22–58). In six of the patients the disease involved the left colon only while the other four had pancolitis. The disease had been present for a mean time of 6.6 years (range 4–11). At the time of biopsy, three patients were receiving only corticosteroids, four were receiving sulphasalazine, and three were not receiving any specific therapy. Based on the criteria established by Truelove and Witts,29 six patients had moderate and four severe disease activity. Table 1 presents clinical characteristics of the patients with ulcerative colitis and Crohn's disease.
Clinical characteristics and treatment of the patients with inflammatory bowel disease at the time of jejunal and colonic biopsies
Seven patients with irritable bowel syndrome were studied as controls. This group consisted of five women and two men, with a mean age of 36 years (range 17–52). None was taking any medication at the time of the study.
In order to analyse OX40+ and OX40L+ cells in the deeper layers of the gut, archival frozen resection samples from children with Crohn's disease were also studied.
Informed consent was obtained from all patients and controls. The study was approved by the Ethical Committee of the University Hospital, Federal University of Rio de Janeiro.
METHODS
Large bowel specimens were obtained by endoscopy of patients under routine examination. Rectal and colonic mucosal biopsy specimens were taken at macroscopically involved areas. The patients with pancolitis showing signs of active inflammation had biopsy specimens taken at the inflamed areas. The same patients had jejunal specimens obtained from the Treitz angle using a Watson capsule under fluoroscopy.
The mucosal samples were immediately covered with OCT compound (Miles Scientific Laboratories Ltd, Naperville, Illinois, USA) and snap frozen in isopentane in a liquid nitrogen bath. They were subsequently stored at −70°C until processing. Sections were first cut at 5 μm in a cryostat maintained at −20°C and were then air dried and fixed for 10 minutes in acetone. Sections of human palatine tonsil were prepared by the same method and were used as positive controls for the immunohistochemical reactions. The cell populations were characterised by indirect alkaline phosphatase immunohistochemistry. Primary antibodies used were anti-CD3 (UCHT-1, Dako Ltd, High Wycombe, Bucks, UK), Act-1 (anti-α4β7), anti-MAdCAM-1, goat polyclonal anti-ICAM-1 (all gifts from Dr A Dogan), and L106 anti-OX40 (a gift from Dr J Shields). Mouse IgG (Dako) was used as a non-specific primary antibody control. Secondary antibodies used were alkaline phosphatase conjugated rabbit antimouse IgG, alkaline phosphatase conjugated goat antirabbit IgG, or a biotinylated rabbit antigoat IgG (all from Dako). The biotinylated rabbit antigoat IgG was detected using alkaline phosphatase conjugated streptavidin (Dako). OX40 ligand expression was detected using an OX40-mouse IgG2a fusion protein (Dr J Shields) and alkaline phosphatase conjugated rabbit antimouse IgG.
Briefly, tissue sections were incubated at room temperature with each antibody or the OX40 mouse IgG2a fusion protein, for at least one hour. Two sections from each patient were incubated with either TBS alone or mouse IgG, and served as negative controls. After rinsing twice in TBS for 10 minutes the sections were incubated for 30 minutes either with a rabbit antimouse alkaline phosphatase conjugate or with a biotinylated rabbit antigoat secondary antibody. The sections incubated with the biotinylated secondary antibody were incubated for 30 minutes with streptavidin-alkaline phosphatase conjugate. The sections incubated either with the Act-1 antibody, the L106 antibody, or with the fusion protein OX40 mouse IgG2a, were submitted to an additional step, being incubated with an alkaline phosphatase conjugated goat antirabbit secondary antibody for 30 minutes to amplify the reaction. Further rinsing was followed by the development with a Fast Red substrate buffer (containing naphtol phosphate, dimethilphormamide, and levamisole).
Preparations were counterstained with Meyer's haemulum and mounted in Aquamount. The sections were examined by a blinded observer under light microscopy. Any lamina propria lymphoid cells or vessels exhibiting identifiable immunoreactivity distinct from background were regarded as positive. Lamina propria positive mononuclear cells and positive vessels were counted in at least six different areas, using a computer assisted image analyser (Seescan, Cambridge, UK). All sections were entirely surveyed using a 10× objective. The results of the quantitative analysis were expressed as either cell or vessel numbers per mm2 lamina propria or submucosa. The optimal dilution of all antibodies was determined using sections of inflamed tonsil.
All statistical analysis was performed using the Mann-Whitney U test. Results are expressed as median values.
Results
EXPRESSION OF CD3+ CELLS
All samples were first stained with the anti-CD3 antibody in order to analyse the number and distribution of T cells in the jejunum and colon. Increased numbers of T cells were seen in the inflamed colonic mucosa from patients with inflammatory bowel diseases compared with the IBS control group. However, no significant difference was seen in the jejunal mucosa of the same individuals (fig 1). No correlation was found between any of the immunohistochemical results and the clinical activity, drug therapy, or endoscopic or histological patterns of inflammatory bowel disease; however, with the relatively small numbers of patients studied, subgroup analysis is difficult.

Density of CD3+ T cells in the lamina propria of the colon (A) and jejunum (B) of controls and patients with inflammatory bowel disease.
EXPRESSION OF ICAM-1
ICAM expression was used as a positive internal control for increased expression of vascular adhesion molecules in the biopsy specimens studied, as its expression is increased in these conditions.1-4 ICAM-1 expression on endothelial cells was significantly increased in the colonic lamina propria of inflammatory bowel disease patients compared with controls, but no significant changes were seen in the jejunal mucosa of the same patients (fig 2).

Density of intercellular adhesion molecule (ICAM) 1+ vessels in the lamina propria of the colon (A) and jejunum (B) of controls and patients with inflammatory bowel disease.
EXPRESSION OF α4β7 AND MAdCAM-1
The integrin α4β7, recognised by the Act-1 antibody, was seen on mononuclear cells of both colonic and jejunal lamina propria in all samples studied. The number of α4β7+ cells was significantly increased in the colonic lamina propria of patients with inflammatory bowel disease compared with IBS controls, but no significant difference was found between patients with ulcerative colitis and Crohn's disease. No significant difference was found between patients with inflammatory bowel disease and IBS controls concerning α4β7 expression on the jejunal mucosa (fig 3). With immunohistochemistry it is not possible to determine how many CD3+ cells coexpressed α4β7, but comparison of relative cell densities in figs 1 and 3 suggested that about one half to one third of the CD3+ cells were α4β7.

Density of α4β7+ cells in the lamina propria of the colon (A) and jejunum (B); and of mucosal addressin cell adhesion molecule (MAdCAM)-1+ vessels in the lamina propria of the colon (C) and jejunum (D) in controls and patients with inflammatory bowel disease.
The expression of MAdCAM-1 was significantly increased in the colonic lamina propria of inflammatory bowel disease patients compared with IBS controls (fig 3), but no significant difference was found between patients with ulcerative colitis and Crohn's disease. There was also no significant difference between inflammatory bowel diseases and controls regarding the expression of MAdCAM-1 on the jejunal mucosa (fig 3).
EXPRESSION OF OX40 AND OX40L
The number of mononuclear cells expressing OX40 in the colonic lamina propria of patients with inflammatory bowel disease was significantly greater than in IBS controls (fig 5). Very few OX40+ mononuclear cells could be identified in the jejunal mucosa, and no significant difference was found between patients and IBS controls (fig5). Compared with the density of α4β7+ cells, OX40+ cells were present at only 10–20% of the density of the former.

Density of OX40+ cells in the lamina propria of the colon (A) and jejunum (B); and of OX40L+ vessels in the colon (C) in controls and patients with inflammatory bowel disease.
The OX40 ligand was seen both on the luminal surface of endothelial cells and mononuclear cells in the lamina propria of the colonic mucosa in patients with IBD (fig 4). Very few vessels stained in IBS patients, and sections from patients with IBD stained with control human IgG also showed no staining. The number of OX40L positive vessels was significantly increased in the colonic mucosa of inflammatory bowel disease patients compared with IBS controls (fig 5). No OX40L positive vessels nor cells could be identified in the jejunal mucosa of either patients or IBS controls (negative data, not shown).
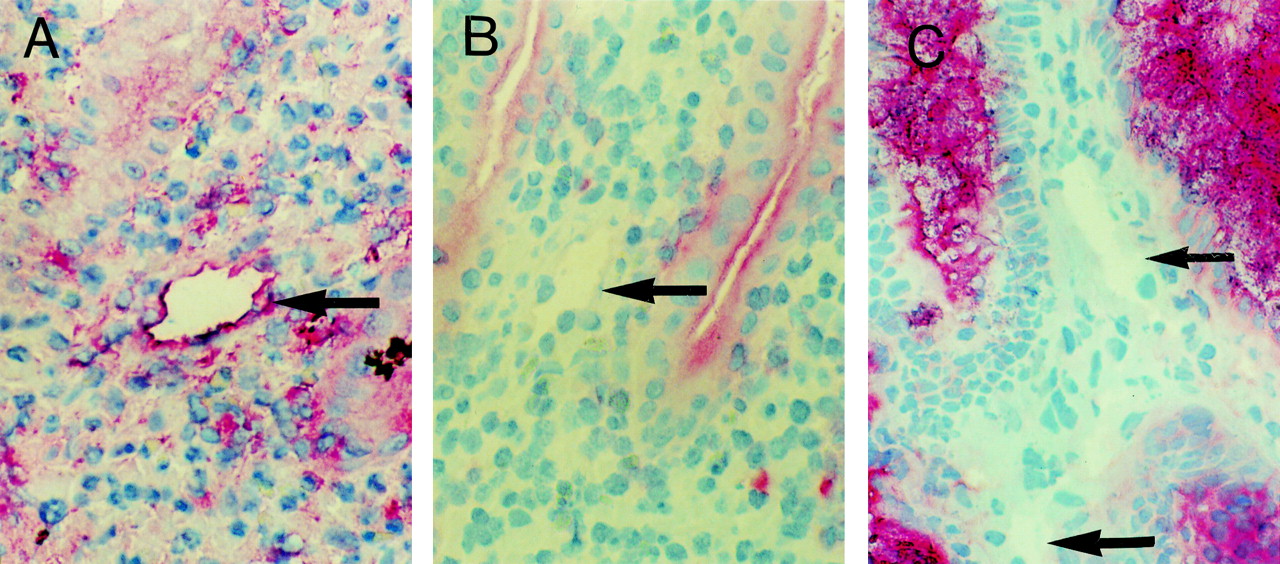
OX40L+ vessels in the colonic mucosa of patients with inflammatory bowel disease. (A) An OX40L+ vessel in the lamina propria of the colon of a patient with ulcerative colitis. (B) Section from a patient with ulcerative colitis which was stained with human control IgG; the vessel is arrowed. (C) Section from the colon of a patient with irritable bowel syndrome stained for OX40L expression. The unstained vessel is also arrowed. The non-specific staining is due to antibody binding to epithelial mucus; this is not seen in A and B because of the mucus depletion associated with ulcerative colitis. Original magnification × 400.
EXPRESSION OF OX40 ON COLONIC MUCOSA AND SUBMUCOSA OF PATIENTS WITH CROHN'S DISEASE
Assessment of the colonic submucosa of patients with Crohn's disease showed that the number of mononuclear cells expressing OX40 receptor was not significantly different from that seen in the lamina propria (fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Density of OX40+ cells in the lamina propria and submucosa of patients with Crohn's disease.
Discussion
The present study has shown an increased expression of α4β7/MAdCAM1 and OX40/OX40 ligand on mononuclear cells and vascular endothelial cells in the colonic mucosa of patients with inflammatory bowel disease, but no significant difference was seen in the jejunal mucosa of the same patients. No obvious correlation was found between the immunohistological results and the clinical or endoscopic characteristics of the patients.
In contrast to other studies on the unaffected mucosa of patients with inflammatory bowel disease, which have detected enhancement of either lamina propria cellular infiltration,30-32 complement secretion,33 or proinflammatory cytokine release,34 we did not find any difference between patients with Crohn's disease, ulcerative colitis, and IBS controls in the number of T cells and in the expression of α4β7/MAdCAM1 and OX40/OX40 ligand in the upper bowel. Earlier studies where increased plasma cells were seen in the upper small bowel of patients with Crohn's disease30 ,31 are difficult to interpret because the role of Helicobacter pylori in gastroduodenal inflammation had not yet been discovered. Other studies34 in which biopsy specimens were taken from endoscopically normal distal bowel of patients with Crohn's disease and increased cytokine production was detected provide stronger evidence of a lesion extending along long stretches of the bowel. However, we are not aware of any study where cytokines have been compared in proximal jejunum of patients with ulcerative colitis or Crohn's colitis.
It is important, however to be clear about what is meant when discussing the extent of Crohn's disease in the bowel. Around 10–12% of patients with distal Crohn's disease have histological lesions in the duodenum.35 ,36 We only analysed nine Crohn's patients, a sample size too small to detect these patients. In this present study, however we were not trying to look at adhesion molecule expression in Crohn's jejunitis, as predictably, it would be increased. Indeed histopathologically, expression in the jejunal biopsy specimens was within the normal range. Instead we were trying to determine whether patients with distal disease had immunological markers of inflammation in the proximal bowel. However, the absence of increased T cell numbers, and vascular adhesion molecules in the jejunum of our patients with inflammatory bowel disease suggests that cytokines may not be increased at distant sites, and that even though there are increased levels of serum cytokines in inflammatory bowel disease, they do not alter vascular adhesion expression at distant sites. Increased vascular adhesion molecule expression is therefore associated with sites of inflammation. Our results on the non-inflamed mucosa do not support the concept of diffuse involvement of the gastrointestinal tract in Crohn's disease, but of course do not preclude the fact that in some patients, upper small bowel disease will develop. In addition, other stigmata of inflammation, not measured in this study, may be present.
Previous studies on vascular endothelial cell surface molecules in inflammatory bowel disease have shown increased numbers of positive vessels and of lamina propria mononuclear phagocytes expressing ICAM-1 in the affected mucosa.2 ,4 Our results with ICAM-1 are in accordance with this. Elevated local cytokine concentrations are almost certainly responsible for the upregulated ICAM-1 in inflammatory bowel disease mucosa.6 ,36-38 However, we included ICAM-1 immunostaining in our study essentially as a positive control against which we could judge endothelial MAdCAM-1 and OX40L expression.
In murine models of inflammatory bowel disease increased expression of MAdCAM-1 is seen in the lamina propria.16-18 The α4β7 integrin is the main ligand for MAdCAM-1, and it defines a subset of CD4+ memory T cells with gut tropism in humans.39Functional data showing inhibition of cell migration to the intestine using antibodies to MAdCAM-1 or anti-α4β7 confirm the importance of the interaction between these molecules to the lymphocyte homing process in the gut.40 In a recent study in intestinal tissue of patients with inflammatory bowel diseases and other inflammatory conditions, and normal controls, it was shown that human MAdCAM-1 is localised to the intestinal mucosa and gut associated lymphoid tissue, and its expression is enhanced in sites of mucosal inflammation.5 The demonstration of the increased expression of α4β7/MAdCAM-1 on the inflamed intestinal mucosa of our patients with inflammatory bowel diseases is in agreement with this work.
The increased expression of OX40+ cells and OX40L+ cells in active colitis is also of interest and to our knowledge has not been studied before. It is noteworthy, however that the density of OX40+ cells was only a fraction of the α4β7+ cells. This probably reflects the fact that in uninflamed intestine, there are many α4β7+ cells whereas there are virtually no OX40+ cells. OX40 may therefore be a better marker of immunopathogenic T cells than α4β7. Recent studies have established that the OX40/OX40L interaction plays an important role in T cell dependent immune response. The OX40/OX40L pair of complementary molecules is a two way signalling system, in which OX40 is present mainly on CD4+ activated T cells, and OX40L on antigen presenting cells.23 The cross linking of the OX40/OX40L molecules has the capacity to costimulate activated T cells, resulting in increased proliferation and cytokine production.41 In an experimental model of autoimmune encephalitis, the OX40 antigen was found to be selectively upregulated on autoreactive T cells isolated from the target organs.42
A subsequent study using the same model showed that when injected in vivo, an OX40 immunotoxin bound exclusively to myelin reactive T cells isolated from the central nervous system and resulted in a better disease outcome.43 The expression of OX40 ligand on human lymphoid and non-lymphoid tissue,41 and more recently on human vascular endothelial cells25 also suggests a possible role in transendothelial migration of activated T cells. The biological importance of OX40/OX40L interactions in bowel inflammation is shown by the fact that treatment of mice with ongoing trinitrobenzene sulphonic acid colitis, or colitic IL-2 knockout mice with an OX40-IgG fusion protein, dramatically inhibits mucosal inflammation, presumably by competitively binding to OX40L on accessory cells and endothelial cells.44 It is not yet known, however whether the OX40-IgG fusion protein is active in vivo because it blocks T cell costimulation, or prevents T cell extravasation into the gut, or both. Interestingly, in the same study in vitro and in vivo there was some evidence that an OX40L-IgG fusion protein enhanced cytokine production and mucosal inflammation, presumably by delivering a costimulatory signal to activated OX40+ CD4+ T cells. Similar protective effects of OX40-IgG treatment on the intestinal phase of graft versus host disease have been reported in mice.45However, in this case, treatment was only successful if given at the same time as infusion of semiallogeneic cells and was unsuccessful if given five days into the response. Inhibition of vascular adhesion molecules and their leucocyte ligands is an attractive notion for a new therapy in Crohn's disease and is effective in animal models. A clinical trial of Act-1 antibody is underway but our results suggest that OX40 might also be a worthwhile target.
Acknowledgments
TT MacDonald is a consultant to Cantab Pharmaceuticals. The authors wish to thank Dr John Shields of Cantab Pharmaceuticals for kindly providing the L106 monoclonal antibody and the OX40 mouse IgG2a fusion protein, and Dr Sylvia Pender for help with the artwork. This work was supported in part by grants from the Brazilian Research Council/CNPq, CAPES, and Fundação José Bonifácio/FUJB.
Abbreviations used in this paper
- IBS
- irritable bowel syndrome
- IL
- interleukin
- TNF
- tumour necrosis factor
- ICAM
- intercellular adhesion molecule
- MAdCAM
- mucosal addressin cell adhesion molecule