


Abstract
Opioid receptor agonists are effective for treating pain; however, tolerance and dependence can develop with repeated use. Combining opioids with cannabinoids can enhance their analgesic potency, although it is less clear whether combined treatment alters opioid tolerance and dependence. In this study, four monkeys received 3.2 mg/kg morphine alone or in combination with 1 mg/kg Δ9-tetrahydrocannabinol (THC) twice daily; the antinociceptive effects (warm water tail withdrawal) of morphine, the cannabinoid receptor agonists WIN 55,212 [(R)-(1)-[2,3-dihydro-5-methyl-3-(4-morpholinylmethyl)pyrrolo[1,2,3-de]-1,4-benzoxazin-6-yl]-1-naphthalenylmethanone mesylate] and CP 55,940 (2-[(1R,2R,5R)-5-hydroxy-2-(3-hydroxypropyl) cyclohexyl]-5-(2-methyloctan-2-yl)phenol), and the κ opioid receptor agonist U-50,488 (trans-3,4-dichloro-N-methyl-N-[2-(1-pyrrolidinyl)-cyclohexyl]benzenacetamide methanesulfonate) were examined before, during, and after treatment. To determine whether concurrent THC treatment altered morphine dependence, behavioral signs indicative of withdrawal were monitored when treatment was discontinued. Before treatment, each drug increased tail withdrawal latency to 20 seconds (maximum possible effect). During treatment, latencies did not reach 20 seconds for morphine or the cannabinoids up to doses 3- to 10-fold larger than those that were fully effective before treatment. Rightward and downward shifts in antinociceptive dose-effect curves were greater for monkeys receiving the morphine/THC combination than monkeys receiving morphine alone. When treatment was discontinued, heart rate and directly observable withdrawal signs increased, although they were generally similar in monkeys that received morphine alone or with THC. These results demonstrated that antinociceptive tolerance was greater during treatment with the combination, and although treatment conditions were sufficient to result in the development of dependence on morphine, withdrawal was not markedly altered by concurrent treatment with THC. Thus, THC can enhance some (antinociception, tolerance) but not all (dependence) effects of morphine.
Introduction
Prescription opioids are widely used for moderate to severe pain; however, increased sales of opioids from 1999 to 2009 were paralleled by increased admissions to substance abuse treatment centers and overdose deaths (Centers for Disease Control and Prevention, 2011). Although prescription opioid abuse has plateaued (Dart et al., 2015), perhaps curtailed by policy and educational initiatives (Brady et al., 2015; Compton et al., 2015; Kanouse and Compton, 2015), the prevalence of prescription opioid use disorders and overdose deaths continues to increase (Han et al., 2015), indicating the need for alternative pharmacotherapies. One treatment approach is to combine opioids with other drugs, such as nonsteroidal anti-inflammatory drugs, in an attempt to retain their analgesic effects while reducing unwanted effects. Although this strategy produces a modest decrease in the opioid dose needed to relieve pain, adverse effects are not markedly changed (Raffa, 2001; Kolesnikov et al., 2003; Raffa et al., 2010; Kao et al., 2012), demonstrating the continuing need for effective and safe drug combinations.
Although combining opioids with a variety of other drugs that have analgesic effects has been considered (e.g., pregabalin and gabapentin; Raffa et al., 2010), mixtures of opioids and cannabinoids seem to be particularly effective at reducing the opioid dose needed to produce antinociceptive effects in rodents (Welch and Stevens, 1992; Welch et al., 1995; Massi et al., 2001; Cichewicz, 2004; Cox et al., 2007; Smith et al., 2007) and monkeys (Li et al., 2008; Maguire et al., 2013) and at increasing the analgesic effectiveness of opioids in pain patients (Narang et al., 2008; Abrams et al., 2011). When given alone, cannabinoid receptor agonists relieve pain under some conditions, and although their own adverse effects might reduce the usefulness of opioid/cannabinoid combinations (Naef et al., 2003; Wang et al., 2008; Pertwee, 2009, 2012; Rahn and Hohmann, 2009), emerging evidence indicates that at least some effects of opioids are not increased, and might even be decreased, by cannabinoids. For example, in monkeys, the discriminative stimulus and reinforcing effects of opioids are not enhanced by cannabinoids (Li et al., 2008, 2012; Maguire et al., 2013), and in humans, there is no difference in adverse effects, such as respiratory or digestive problems, when a combination of morphine and Δ9-tetrahydrocannabinol (THC) is compared with either drug given alone (Naef et al., 2003). Thus, although antinociceptive effects of opioids are increased by cannabinoids, not all effects are similarly changed, suggesting an improved margin of safety for opioid/cannabinoid combinations.
Although acute adverse effects are important clinically, chronic pain requires long-term treatment. Consequently, the possible development of tolerance and dependence with repeated administration is a concern when developing novel drug mixtures for treating pain. These adverse effects are particularly important for opioid/cannabinoid combinations because cross-tolerance develops between these two drug classes. For example, the antinociceptive potency of cannabinoids is decreased in morphine-tolerant monkeys (Gerak et al., 2015) and in some morphine-tolerant rats (Basilico et al., 1999; Yesilyurt and Dogrul, 2004; Maguma and Taylor, 2011). When opioids and cannabinoids are combined, tolerance and cross-tolerance might develop concurrently and produce a greater decrease in antinociceptive potency than would be observed when either drug is given alone; however, some studies in rodents receiving morphine and cannabinoids concurrently report that antinociceptive tolerance is not greater for the combination (Cichewicz and Welch, 2003; Smith et al., 2007; Fischer et al., 2010). The goal of the current study was to determine whether THC alters tolerance to and dependence on morphine in monkeys. Tolerance was assessed by determining changes in potency of the opioids morphine and U-50,488 (trans-3,4-dichloro-N-methyl-N-[2-(1-pyrrolidinyl)-cyclohexyl]benzenacetamide methanesulfonate) and the cannabinoids WIN 55,212 [(R)-(1)-[2,3-dihydro-5-methyl-3-(4-morpholinylmethyl)pyrrolo[1,2,3-de]-1,4-benzoxazin-6-yl]-1-naphthalenylmethanone mesylate] and CP 55,940 (2-[(1R,2R,5R)-5-hydroxy-2-(3-hydroxypropyl) cyclohexyl]-5-(2-methyloctan-2-yl)phenol) using a warm-water tail withdrawal procedure in monkeys. Although THC is used clinically, it has a slow onset and long duration of action, making it difficult to obtain an entire dose-effect curve in a single session (Ginsburg et al., 2014; Hruba and McMahon, 2014; Maguire and France, 2014). Because of their pharmacokinetics, dose-effect curves could more easily be determined within a session for two other cannabinoid receptor agonists: WIN 55,212 and CP 55,940. Dependence was evident by the emergence of withdrawal when treatment was discontinued; a number of withdrawal signs were monitored, including changes in heart rate, body temperature, activity, and directly observable signs (e.g., unusual tongue movement; Gerak et al., 2015).
Materials and Methods
Subjects.
Four adult rhesus monkeys were housed in individual cages and maintained on a 14-/10-hour light/dark cycle. Before chronic treatment began, the two male monkeys (subjects LO and BU) weighed 8.4 and 7.7 kg, respectively, and the two female monkeys (subjects RE and CL) weighed 8.8 and 8.0 kg, respectively. Monkeys had unlimited access to water and were provided with a daily ration of monkey chow (High Protein Monkey Diet; Harlan Teklad, Madison, WI) and fresh fruit. Monkeys were maintained in accordance with the Institutional Animal Care and Use Committee (The University of Texas Health Science Center, San Antonio, TX) and the 2011 Guide for the Care and Use of Laboratory Animals (Institute of Laboratory Animal Resources on Life Sciences, National Research Council, National Academy of Sciences, Washington, DC).
Surgery.
Monkeys were anesthetized with 100 mg of ketamine followed by intubation and maintenance with 2.5% isoflurane (Gerak et al., 2015). Telemetry devices (model CTA-D70; Data Science International, Arden Hills, MN) were placed in the right flank with positive ECG leads tunneled to the lower-left quadrant of the thorax and negative ECG leads tunneled to the upper-right quadrant. Absorbable suture (Ethicon Inc., Somerville, NJ) was used to close muscle, tissue, and skin incision sites. Monkeys received meloxicam and penicillin B&G (40,000 IU/kg) postoperatively and were not tested for at least 1 week after surgery.
Apparatus.
Antinociception studies were conducted while monkeys were seated in chairs (Primate Products, Miami, FL). Latency to remove tails from insulated mugs containing water at 50, 54, or 58°C was measured using a stopwatch. Signals were sent from activated telemetry devices to receivers (model RMC-1; Data Science International, Arden Hills, MN) attached to home cages. A computer used Dataquest A.R.T. software (Data Science International) to convert the signals to heart rate (beats per minute), body temperature (°C), and activity (counts per minute).
Antinociception.
A warm-water tail withdrawal procedure was used to assess antinociception (Gerak et al., 2015). The lower portion of the shaved tail was placed in water maintained at 50, 54, and 58°C, and the latency to remove the tail from the water was measured. The order of presentation of the temperatures varied nonsystematically across cycles and across monkeys. Experimental sessions were divided into cycles that began with an injection of vehicle or drug and ended with assessment of latency. The antinociceptive effects of four drugs were determined before, during, and after chronic treatment: the µ opioid receptor agonist morphine, the κ opioid receptor agonist U-50,488, and the cannabinoid receptor agonists WIN 55,212 and CP 55,940. The κ opioid receptor agonist U-50,488 was included because it has antinociceptive effects in monkeys; however, cross-tolerance does not develop during chronic treatment with μ opioid receptor agonists (Brandt and France, 2000), and the potency of U-50,488 would not be expected to change during chronic treatment with morphine and THC. Dose-effect curves were determined by increasing the cumulative dose across cycles which varied in length across sessions depending on the drug being studied. After an initial determination of tail-withdrawal latency at each temperature, saline was administered and latency was obtained again 13 minutes later. Monkeys received the first injection of drug 15 minutes after the injection of saline. Thereafter, injections were given every 15 minutes when dose-effect curves for the opioids were generated, with latencies determined 13 minutes after each drug injection or every 30 minutes when dose-effect curves for the cannabinoids were generated with latencies determined 28 minutes after each drug injection (Gerak et al., 2015). The smallest dose studied was ineffective, with the cumulative dose increasing in 1/4 log unit increments across cycles until a latency of 20 seconds was obtained at 54°C or up to a maximum dose of 32 mg/kg morphine, 3.2 mg/kg U-50,488, 5.6 mg/kg WIN 55,212, or 0.56 mg/kg CP 55,940. At least 7 days separated determination of a cannabinoid dose-effect curve from the next drug test.
Behavioral Observations.
Two individuals monitored directly observable signs at 0930 hours. Monkeys remained in their home cage while the observers recorded the presence or absence of 15 signs (listed in Table 1 in Becker et al., 2008) that have been reported during withdrawal from μ opioid receptor agonists in nonhuman primates (Light and Torrance, 1929; Kleber et al., 1980; Katz, 1986; Sell et al., 2005; Li et al., 2007; Becker et al., 2008; Gerak et al., 2015). Monkeys were observed for 15 seconds of every minute for eight consecutive minutes, resulting in a maximum possible frequency score of 8 for each sign. The observers were experienced and acquainted with the behavior of these particular monkeys. One of the two observers administered drug and was not blind to treatment, although both observers were blind to the purpose and expected outcomes of the experiment.
Telemetry Procedure.
Transmitters were activated before treatment, periodically during treatment, and continuously after termination of treatment to monitor heart rate, body temperature, and activity. For each dependent variable, 10 data points were obtained during each hour by collecting data continuously for 60-second periods that were separated by 5-minute intervals, during which data were not collected.
Chronic Morphine Treatment.
Once the acute antinociceptive effects of morphine, U-50,488, WIN 55,212, and CP 55,940 were determined, chronic morphine administration began. There were two distinct periods of chronic morphine treatment that were identical, except for the solution administered concurrently with each injection of morphine. During the first treatment period, 1 mg/kg THC was administered with morphine, whereas during the second treatment period, vehicle was administered with morphine. Although the dose of THC remained the same throughout treatment, the initial morphine dose was small (1 mg/kg/day) and increased systematically across days until monkeys were receiving 3.2 mg/kg morphine twice daily (at 0700 and 1700 hours); this dosing regimen has been reported previously (Gerak et al., 2015). The final dosing conditions were achieved on day 10 of treatment.
Dose-effect curves for antinociception were determined periodically during treatment. On the day of the test, vehicle replaced drug at 0700 hours, and determination of the dose-effect curve began at 1000 hours; thus, tests were conducted 17 hours after the last morphine injection, given with THC during the first treatment period and given alone during the second treatment period. Vehicle was administered after the test session at 1700 hours due to the large doses of drug studied during the session; twice-daily treatment resumed at 0700 hours on the day after determination of the dose-effect curve for antinociception and continued uninterrupted until the next test.
The antinociceptive effects of morphine were determined on day 13 of treatment; thereafter, dose-effect curves were generally obtained once per week with at least 7 days separating a cannabinoid dose-effect curve from the next drug test. During chronic treatment, morphine dose-effect curves were generated four times, whereas dose-effect curves for each of the other three drugs were determined once. The order of testing during chronic treatment is shown in Table 1, and the order of testing after treatment was discontinued is shown in Table 2.
Testing schedule during chronic treatment
The order of testing was the same when monkeys received the morphine/THC combination and when they received morphine alone.
Testing schedule after discontinuation of chronic treatment
The order of testing was the same after the two treatment periods.
Each period of chronic treatment lasted 80 days. When drug treatment was terminated, vehicle injections replaced drug injections at 0700 and 1700 hours for 3 weeks, during which time telemetry devices were continuously activated, observations were conducted at least twice weekly at 0930 hours, and morphine dose-effect curves were determined weekly beginning 7 days after the last day of treatment. Twice-daily injections of vehicle stopped after 3 weeks, although physiologic and directly observable signs continued to be recorded at least twice each week, and cannabinoid dose-effect curves were determined every other week (WIN 55, 212 during weeks 4 and 10; CP 55,940 during weeks 6 and 8). The U-50,488 dose-effect curve was obtained 9 weeks after the last treatment dose was administered.
During the first treatment period, the combination of morphine and THC was administered chronically. Daily administration of morphine alone began 102 days after the last day of treatment with the combination of morphine and THC. Before beginning treatment with morphine alone, telemetry devices with fully charged batteries were implanted. Other than the concurrent administration of THC, the two treatment periods were identical.
Drugs.
Morphine sulfate, THC (100 mg/ml in absolute ethanol), CP 55,940 (2-[(1R,2R,5R)-5-hydroxy-2-(3-hydroxypropyl) cyclohexyl]-5-(2-methyloctan-2-yl)phenol; 10 mM in absolute ethanol), and U-50,488 methanesulfonate (trans-3,4-dichloro-N-methyl-N-[2-(1-pyrrolidinyl)-cyclohexyl]benzenacetamide methanesulfonate) were provided by the Research Technology Branch, National Institute on Drug Abuse (Rockville, MD). WIN 55,212 mesylate [(R)-(1)-[2,3-dihydro-5-methyl-3-(4-morpholinylmethyl)pyrrolo[1,2,3-de]-1,4-benzoxazin-6-yl]-1-naphthalenylmethanone mesylate] was purchased from Tocris (Ellisville, MO). Morphine and U-50,488 were dissolved in sterile water. A 1:1:18 mixture of ethanol, Emulphor-620 (Rhone-Poulenc Inc., Princeton, NJ), and 0.9% saline was used to dilute CP 55,940 and dissolve WIN 55,212. Injections were given s.c. in a volume of 0.1–1.0 ml.
Data Analyses.
GraphPad Prism version 6.03 for Windows (GraphPad Software, La Jolla, CA) was used for analyzing and graphing data, which were averaged across the four monkeys (±1 S.E.M.) and plotted as a function of dose (antinociception), treatment condition (area under antinociception dose-effect curves), or time since the last day of treatment (physiologic and directly observable withdrawal signs). ED50 values could not be obtained during chronic treatment because the latency to withdrawal the tail did not exceed 50% of the maximum possible latency (i.e., 20 seconds) from 54°C water for some monkeys up to the largest doses of morphine, WIN 55,212, and CP 55,940 studied. Even when tail-withdrawal latencies increased such that ED50 values could be estimated, slopes of the dose-effect curves were significantly different across treatment conditions, thereby precluding comparisons of ED50 values. Those limitations were circumvented by calculating the area under the dose-effect curve (AUC) and comparing those values across treatment conditions (Gerak et al., 2015); however, to use this approach, an important assumption was necessary because it was not possible to study an identical dose range for a particular drug across the different treatment conditions. For example, the largest doses of morphine studied in morphine-tolerant monkeys could not be safely administered to nontolerant monkeys. Consequently, for the AUC analyses, the dose range for each drug was standardized across treatment conditions by assuming that doses smaller than an ineffective dose were also ineffective, and a latency of 1 second was assigned to doses smaller than the first dose given. Similarly, doses larger than those studied were assumed to be maximally effective and were assigned a latency of 20 seconds, thereby providing the most conservative estimate of tolerance. With this strategy, latencies were assigned or measured for every dose within the same range of doses for a particular drug for all treatment conditions. The dose ranges used to calculate AUC values were 0.178–32 mg/kg for morphine; 0.56–3.2 mg/kg for U-50,488; 0.1–5.6 mg/kg for WIN 55,212; and 0.01–0.56 mg/kg for CP 55,940. AUC values could then be compared using a one-factor (treatment condition), Geisser-Greenhouse corrected repeated-measures analysis of variance (ANOVA) followed by Dunnett’s multiple comparisons test, which compared AUC values obtained during and after treatment with morphine alone and in combination with THC to AUC values obtained for that drug before any treatment. Significance was set at P < 0.05.
Heart rate, body temperature, and activity were recorded 10 times per hour throughout the day and night. For each dependent variable, data for individual monkeys were averaged to obtain one value per hour. Because there was no significant difference across daytime or across nighttime hours in any telemetry measure in these monkeys (Gerak et al., 2015), and because the animals were generally cared for during the 4 hours after the room lights were illuminated for the day, data for each hour were averaged across the 10-hour nighttime period (2000–0600 hours) and across the last 10 hours of the daytime period (1000–2000 hours). The dependent variables were analyzed separately using two-factor (time since last injection, day/night) repeated-measures ANOVA followed by Dunnett’s multiple comparisons test to compare data obtained on a single treatment day and on each withdrawal day with data obtained on a single day before treatment began. Sidak’s multiple comparisons test was used to compare withdrawal signs after termination of morphine given in combination with THC to those that emerge after termination of morphine given alone.
Directly observable signs were analyzed individually and combined to give a composite score for total withdrawal signs. For each sign, the frequency with which it occurred was averaged among monkeys (±1 S.E.M.); any signs that occurred during more than one observation period on at least 1 day of withdrawal were analyzed using a one-factor (treatment condition) repeated-measures ANOVA. No further analyses were conducted on individual signs that rarely occurred (e.g., emesis, salivation), although all 15 signs were combined to obtain a total withdrawal score. This composite score was determined by adding the frequency of the individual signs across each 8-minute observation period. Although the maximum possible score for total withdrawal signs was 120 (maximum frequency of 8 for each of the 15 signs scored), the actual composite score was much lower because of the large number of signs that were never observed. Reliability between observers was assessed using the κ statistic, which was determined for the composite score of total withdrawal signs and considered adequate when κ was greater than 0.80 (Landis and Koch, 1977; Hallgren, 2012).
Results
Acute Antinociceptive Effects of Opioids and Cannabinoids.
Before chronic treatment, administration of saline resulted in average tail-withdrawal latencies of 15.3 ± 4.8 seconds in 50°C water and 1 second in 54 and 58°C water. In otherwise untreated monkeys, each of the four test drugs dose dependently increased latencies to the maximum of 20 seconds in 50 (data not shown) and 54°C water (Figs. 1 and 2, squares). CP 55,940 was the most potent of the four drugs, with a maximum possible effect occurring at a cumulative dose of 0.178 mg/kg in 54°C water, followed by WIN 55,212 (1 mg/kg), U-50,488 (1.78 mg/kg), and morphine (3.2 mg/kg). The effects of these drugs were temperature-dependent, with monkeys removing their tails in 4 seconds or less from 58°C water (data not shown) at doses of each drug that produced 20-second latencies at 54°C.

Antinociceptive effects of morphine (left panels) and U-50,488 (right panels) in four monkeys before, during, and after chronic treatment with morphine alone or in combination with THC. (Top) Dose-effect curves determined before chronic treatment (squares) and on the 55th day of twice-daily treatment with either 3.2 mg/kg morphine alone (circles) or 3.2 mg/kg morphine and 1 mg/kg THC (triangles). (Second from top) Dose-effect curves determined before chronic treatment (squares, same curve as in top panel), on the 55th day of twice-daily treatment with 3.2 mg/kg morphine and 1 mg/kg THC (triangles, same curve as in top panel), and after discontinuation of treatment with the morphine/THC combination (half-filled triangles). (Second from bottom) Dose-effect curves determined before chronic treatment (squares, same curve as in top panel), on the 55th day of twice-daily treatment with 3.2 mg/kg morphine alone (circles, same curve as in top panel), and after discontinuation of treatment (half-filled circles). (Bottom) Area under dose-effect curves determined before (squares), during (triangles, circles), and after treatment (half-filled symbols). For clarity, morphine dose-effect curves determined 1 and 2 weeks after termination of treatment are not plotted in the middle panels (see lower panel). *The AUC is statistically different from the AUC obtained before chronic treatment. Ordinates: top three rows, latency (seconds) to remove tails from 54°C water averaged across monkeys (±S.E.M.); bottom, AUC. Abscissae: top 3 rows, saline (S) or opioid dose in milligrams per kilogram of body weight; bottom panels, morphine treatment condition (weeks 1, 2, 3, and 9 indicate the number of weeks since discontinuation of treatment).

Antinociceptive effects of WIN 55,212 (left) and CP 55,940 (right) in four monkeys before, during, and after chronic treatment with morphine alone or in combination with THC. (Top) Dose-effect curves determined before chronic treatment (squares) and on the 55th day of twice-daily treatment with either 3.2 mg/kg morphine alone (circles) or 3.2 mg/kg morphine and 1 mg/kg THC (triangles). (Second from top) Dose-effect curves determined before chronic treatment (squares, same curve as in top panel), on the 55th day of twice-daily treatment with 3.2 mg/kg morphine and 1 mg/kg THC (triangles, same curve as in top panel), and after discontinuation of treatment (half-filled triangles). (Second from bottom) Dose-effect curves determined before chronic treatment (squares, same curve as in top panel), on the 55th day of twice-daily treatment with 3.2 mg/kg morphine alone (circles, same curve as in top panel), and after discontinuation of treatment (half-filled circles). (Bottom) Area under dose-effect curves determined before (squares), during (triangles, circles), and after treatment (half-filled symbols). For clarity, cannabinoid dose-effect curves determined 4 and 6 weeks after termination of treatment are not plotted in the middle panels (see lower panel). *The AUC is statistically different from the AUC obtained before chronic treatment. Ordinates: top three rows, latency (seconds) to remove tails from 54°C water averaged across monkeys (±S.E.M.); bottom, AUC. Abscissae: top three rows, saline (S) or cannabinoid dose in milligrams per kilogram of body weight; bottom panels, morphine treatment condition (weeks 4, 6, 8, and 10 indicate the number of weeks since discontinuation of treatment).
Antinociceptive Effects of Morphine during Chronic Treatment: Decreased Potency and the Development of Opioid Tolerance and Cannabinoid Cross-Tolerance.
Chronic treatment with morphine either alone or in combination with THC decreased the potency of morphine. In monkeys receiving 3.2 mg/kg morphine twice daily, the morphine dose-effect curve determined 17 hours after the last treatment dose was shifted 10-fold rightward, and up to a dose of 32 mg/kg, three of the four monkeys left their tails in water maintained at 54°C for at least 15 seconds (Fig. 1, circles, upper-left panel). During treatment with a combination of 3.2 mg/kg morphine and 1 mg/kg THC, the morphine dose-effect curve was shifted further to the right, as compared with the curve obtained during treatment with morphine alone, and only one of the four monkeys left its tail in 54°C water for at least 15 seconds at a cumulative dose of 32 mg/kg morphine (Fig. 1, triangles, upper-left panel). The change in potency of morphine that occurred during chronic treatment was reversed when treatment was discontinued (Fig. 1, middle-left panels). Three weeks after morphine/THC treatment ended, the morphine dose-effect curve was shifted slightly to the right of the curve obtained before chronic treatment, with a mean latency of 15.7 seconds at a cumulative dose of 3.2 mg/kg (Fig. 1, half-filled triangles, left panels). After discontinuation of treatment with morphine alone, the morphine dose-effect curve remained 3-fold to the right of the curve obtained before treatment, with a mean latency of 12.7 seconds at a cumulative dose of 3.2 mg/kg (Fig. 1, half-filled circles, left panels). The area under the morphine dose-effect curve was significantly changed by chronic treatment (F10,30 = 6.22, P = 0.042); post hoc analyses revealed a significant difference between the AUC obtained during combined treatment with morphine and THC and the AUC obtained before treatment (Fig. 1, bottom-left panel). AUC was not significantly different across the first 3 weeks after discontinuation of either period of chronic treatment, as compared with the AUC obtained before chronic treatment.
Antinociceptive Effects of U-50,488 during Chronic Treatment: No Change in Potency Demonstrating No Cross-Tolerance.
In contrast, the potency of U-50,488 was not significantly changed during chronic treatment. There was a modest rightward shift in the U-50,488 dose-effect curve that was similar during both periods of chronic treatment (Fig. 1, upper-right panel). In one monkey receiving the morphine/THC combination, tail-withdrawal latency could not be obtained after a cumulative dose of 3.2 mg/kg due to safety concerns, and doses larger than 3.2 mg/kg were not given. A latency of 20 seconds was obtained with 1.78 mg/kg U-50,488 before chronic treatment, and this dose produced latencies of 13.6 and 11.3 seconds during treatment with the morphine/THC combination and with morphine alone, respectively. Although the potency of U-50,488 did not change markedly 9 weeks after discontinuation of treatment, 3.2 mg/kg could be safely administered and 20-second latencies were obtained in all four monkeys (Fig. 1, middle-right panels). The area under the U-50,488 dose-effect curve was not significantly changed by chronic treatment (F4,12 = 4.92, P = 0.068; Fig. 1, bottom-right panel).
Antinociceptive Effects of Cannabinoids during Chronic Treatment: Decreased Potency Demonstrating Cannabinoid Tolerance and Opioid Cross-Tolerance.
Changes in the antinociceptive effects of the cannabinoids during twice-daily administration of morphine alone or with THC resembled changes observed in the antinociceptive effects of morphine. Treatment with morphine alone shifted the WIN 55,212 dose-effect curve 3-fold rightward, with a mean latency of 15.3 seconds at 1.78 mg/kg (Fig. 2, circles, upper-left panel); when morphine was given with THC, the shift was even larger, and up to a dose of 5.6 mg/kg WIN 55,212, mean latency did not exceed 5 seconds (Fig. 2, triangles, upper-left panel). Chronic treatment also shifted the CP 55,940 dose-effect curve rightward, although there was little difference between dose-effect curves obtained during twice-daily treatment with morphine alone and those obtained during treatment with the combination, and mean latencies were greater than 15 seconds at all doses studied (Fig. 2, upper-right panel). When chronic treatment with the morphine/THC combination was discontinued, the change in potency of both cannabinoids was reversed, with dose-effect curves similar to those obtained before chronic treatment (Fig. 2, half-filled triangles, middle panels). Although the dose of WIN 55,212 (1 mg/kg) needed to increase the mean latency to at least 15 seconds was the same before and after treatment with the combination, a 3-fold larger dose of CP 55,940 was needed to increase the mean latency to at least 15 seconds (before, 0.1 mg/kg; after, 0.32 mg/kg). After the second period of chronic treatment, during which morphine was given alone, the change in potency was not reversed. Dose-effect curves were more similar to those obtained during treatment, as compared with before treatment, and mean latency did not exceed 15 seconds at any dose tested (Fig. 2, half-filled circles, middle panels). Chronic treatment significantly changed the AUC for WIN 55,212 (F6,18 = 6.20, P = 0.047) and CP 55,940 (F6,18 = 11.05, P = 0.007). For both drugs, post hoc analyses revealed a significant difference between the AUC obtained during chronic treatment with the combination and the AUC obtained before chronic treatment. After treatment, dose-effect curves for the cannabinoids were determined twice, and the AUCs obtained after chronic treatment were not significantly different from the curves obtained before chronic treatment; however, for both cannabinoids, the AUCs increased over time since discontinuation of treatment with the combination and decreased over time since discontinuation of treatment with morphine alone.
Physiologic Withdrawal Signs.
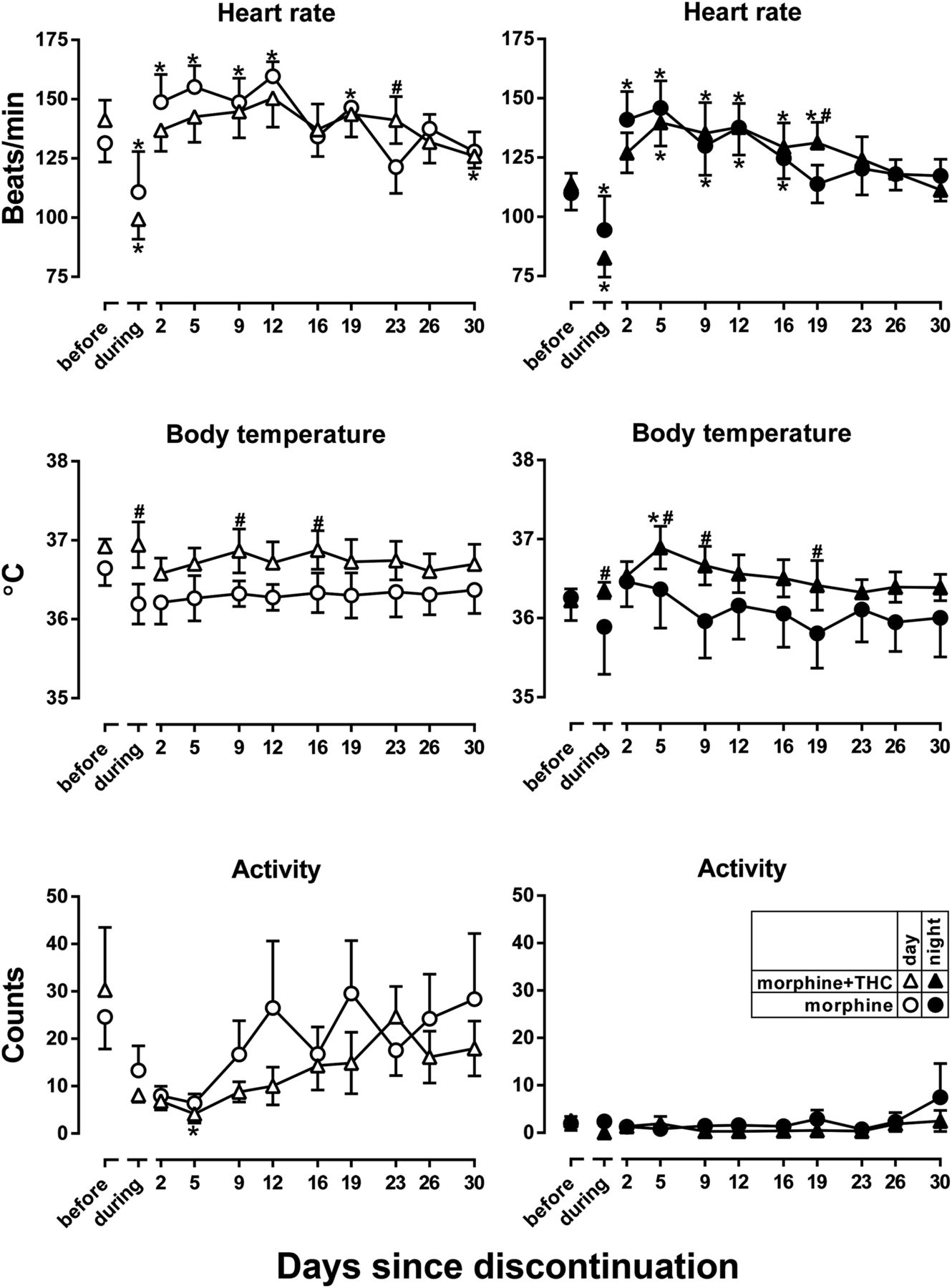
Withdrawal signs emerged when drug treatment was discontinued, although combined morphine/THC treatment did not reliably alter the magnitude or persistence of these signs. Chronic morphine treatment, either alone or with THC, significantly changed heart rate (Fig. 3, top panels) with significant main effects of days since treatment (F12,36 = 9.46, P < 0.0001) and time of day (day vs. night; F3,9 = 11.69, P = 0.0019) and a significant interaction between those factors (F36,108 = 3.77, P < 0.0001). Before morphine treatment, heart rate was decreased overnight as compared with heart rate during the day. Chronic treatment with morphine, whether it was given alone or in combination with THC, significantly decreased both daytime and nighttime heart rate (Fig. 3, points above “during,” upper panels; data marked with * indicate that heart rate is significantly different from heart rate before treatment). Discontinuation of treatment with morphine alone significantly increased heart rate during the day and overnight as compared with heart rates obtained before chronic treatment; the increase in nighttime heart rate lasted longer than the increase in daytime heart rate (19 vs. 12 days). Treatment with a combination of morphine and THC did not significantly increase daytime heart rate over the first 26 days after discontinuation of treatment. Although nighttime heart rate was increased after discontinuation of the combination, the effect did not emerge until 5 days after discontinuation and was gone within 19 days of the last treatment. Significant differences between the two treatment periods were evident only during the daytime on discontinuation day 23 and during the nighttime on discontinuation day 19 (Fig. 3, upper panels; data marked with # indicate that heart rate obtained during or after treatment with the combination is significantly different from heart rate obtained during or after treatment with morphine alone).

Heart rate (top), body temperature (middle), and activity (bottom) in untreated monkeys (points above “before”), during treatment with 3.2 mg/kg morphine alone or in combination with 1 mg/kg THC (points above “during”), and after discontinuation of treatment. Data obtained during the light cycle (i.e., 1000–2000 hours) are shown in the left panels, and data obtained during the dark cycle (i.e., 2000–0600 hours) are shown in the right panels. *The point is significantly different from the point obtained before chronic treatment; #The point obtained during or after treatment with the combination is significantly different from the point obtained during or after treatment with morphine alone. Ordinates: upper panel, heart rate (beats per minute); middle panel, body temperature (°C); bottom panel, activity (counts per minute). Abscissa: days since discontinuation of treatment.
Body temperature was significantly different in monkeys receiving the morphine/THC combination chronically, as compared with monkeys receiving chronic treatment with morphine alone (Fig. 3, middle panels). There was a main effect of time of day (day vs. night; F3,9 = 5.42, P = 0.021) and an interaction between days since treatment and time of day (F36,108 = 2.41, P = 0.0003). Nighttime body temperature was significantly increased 5 days after the last administration of the combination of morphine and THC as compared with values obtained before treatment (Fig. 3, middle panels; data marked with * indicate that body temperature is significantly different from body temperature before treatment). During chronic treatment, daytime and nighttime body temperatures were significantly higher in monkeys receiving the morphine/THC combination as compared with monkeys receiving morphine alone (Fig. 3, points above “during,” middle panels; data marked with # indicate that body temperature obtained during or after treatment with the combination is significantly different from body temperature obtained during or after treatment with morphine alone); in addition, there were a few instances after discontinuation of treatment when body temperature in monkeys that had received the combination was higher than body temperature in monkeys that received morphine alone.
Activity was also changed as a result of daily administration of morphine with and without THC (Fig. 3, bottom panels). There were significant main effects of days since treatment (F12,156 = 2.14, P = 0.018) and time of day (day vs. night; F3,156 = 34.29, P < 0.0001), although there was no interaction between those factors. Daytime activity was significantly decreased 5 days after the last administration of the combination (Fig. 3, bottom panels; data marked with * indicate that activity is significantly different from activity before treatment). Activity was not significantly different between monkeys receiving morphine alone and monkeys receiving the combination.
Directly Observable Withdrawal Signs.
Discontinuation of morphine treatment also increased directly observable signs that are characteristic of opioid withdrawal (Fig. 4). Agreement between raters of directly observable signs was found to be adequate, with κ = 0.91. Only one sign, out of the 15 that were monitored, was significantly increased during withdrawal, with main effects of days since treatment (F7,21 = 7.61, P = 0.0001) and treatment drug(s) (F1,3 = 11.22, P = 0.044), although there was no interaction between these factors. This sign, unusual tongue movement, was not evident before or during treatment with morphine alone or in combination with THC and increased when either treatment period ended (Fig. 4, bottom panel). Although there was not a significant difference in unusual tongue movement between the two treatment periods, this withdrawal sign emerged sooner when morphine/THC treatment was discontinued, as compared with discontinuation of treatment of morphine alone. When the 15 signs were combined into a single withdrawal score, there were significant main effects of days since treatment (F7,21 = 6.73, P = 0.0003) and treatment drug(s) (F1,3 = 20.95, P = 0.020) and no interaction between these factors. During treatment, withdrawal signs were not different from before treatment and increased significantly when both treatment periods ended (Fig. 4, top panel). Withdrawal signs were significantly greater on discontinuation day 7 and lasted longer when treatment with the combination was discontinued, as compared with discontinuation of morphine alone.
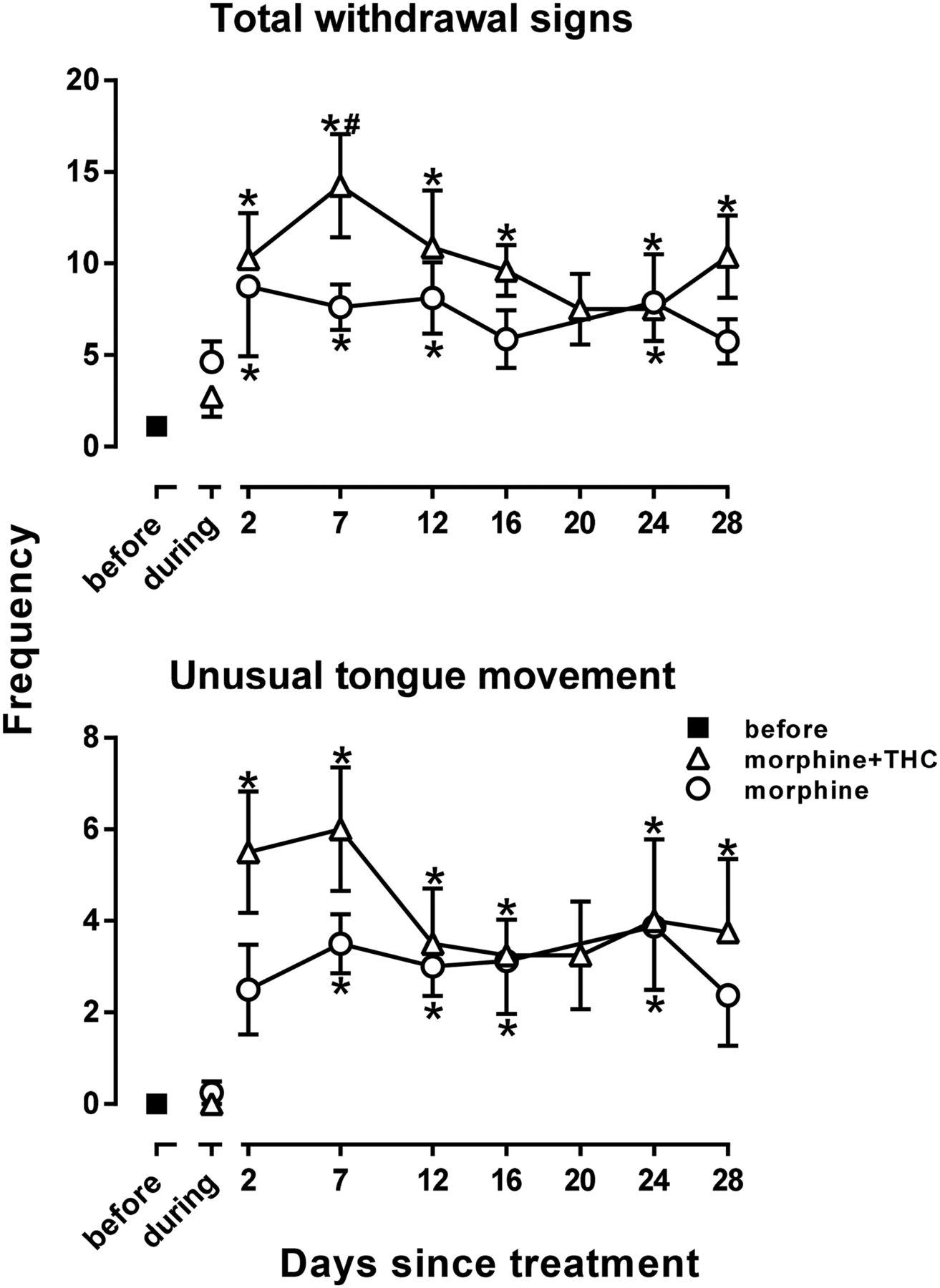
Total withdrawal signs (top) and unusual tongue movement (bottom) in untreated monkeys (points above “before”), during treatment with 3.2 mg/kg morphine alone or in combination with 1 mg/kg THC (points above “during”), and after discontinuation of treatment. Total withdrawal signs are a composite score of withdrawal determined by adding the frequency of the individual signs across each 8-minute observation period. Unusual tongue movement was the only sign that was significantly different during withdrawal, and therefore, it is the only sign plotted. *The point is significantly different from the point obtained before chronic treatment; #The point obtained after treatment with the combination is significantly different from the point obtained after treatment with morphine alone. Ordinates: frequency. Abscissa: days since discontinuation of treatment.
Discussion
Prescription opioids effectively treat moderate to severe pain in many, but not all, patients; however, there has been an exponential increase in abuse of these drugs and a concomitant increase in overdose deaths, resulting in the current epidemic that has not been fully addressed by changes in policy and educational initiatives. One approach that might slow down this epidemic is to develop novel pharmacotherapies for pain that are as effective as opioids and less likely to be abused. Combining opioids and cannabinoids has been shown to markedly reduce the dose of opioid needed for antinociceptive effects (Welch and Stevens, 1992; Welch et al., 1995; Massi et al., 2001; Cichewicz, 2004; Cox et al., 2007; Smith et al., 2007; Li et al., 2008; Maguire et al., 2013). Ongoing research is determining whether cannabinoids enhance other clinically unwanted effects of opioids in addition to their antinociceptive effects, and initial studies suggest that abuse-related effects of opioids are not increased by cannabinoids in monkeys (Li et al., 2008, 2012; Maguire et al., 2013). Given the clinical need for effective and safe treatments for chronic pain, the aim of the current study was to determine whether concurrent administration of the cannabinoid THC alters the development of antinociceptive tolerance to and dependence on morphine, two important adverse effects that can occur when opioids are used chronically.
Although concurrent administration of THC had a minimal impact on morphine dependence, as evidenced by the emergence of withdrawal when treatment was discontinued, tolerance was greater when THC and morphine were combined. In rhesus monkeys receiving twice-daily treatment with 3.2 mg/kg morphine alone, tolerance to morphine and cross-tolerance to cannabinoids developed; the AUC for each drug was similar across different periods of chronic treatment with this morphine dose (current study; Gerak et al., 2015), demonstrating the reliability and repeatability of this effect. When 1 mg/kg THC was added to the treatment regimen, tolerance to cannabinoids and cross-tolerance to morphine developed, as evidenced by greater shifts to the right in the antinociceptive dose-effect curves for morphine and WIN 55,212. The potency of the κ opioid receptor agonist U-50,488 was not markedly changed during chronic treatment with morphine given either alone or with THC, demonstrating that the development of tolerance and cross-tolerance was selective for drugs acting at μ opioid receptors and cannabinoid receptors. When given acutely, 1 mg/kg THC, which did not alter tail withdrawal latency at 54°C in the absence of other treatment, significantly increased the potency of opioids to produce antinociceptive effects (Maguire and France, 2014). Thus, an ineffective dose of THC enhanced both the antinociceptive effects of and the development of tolerance to morphine.
The greater tolerance and cross-tolerance that occurs in monkeys receiving opioids and cannabinoids concurrently is opposite to those effects obtained in rodents. For example, daily treatment with morphine alone or THC alone decreases their antinociceptive effectiveness in rats; when given together, smaller doses of each drug are needed to produce antinociception, and tolerance to the mixture does not develop (Smith et al., 2007). One difference between that study and the current study is that the treatment dose of morphine used in rats was smaller when it was combined with THC, as compared with the treatment dose of morphine administered alone. In the current study in monkeys, the treatment dose of morphine was the same when it was given alone or in combination with THC, and the use of this relatively larger treatment dose, which was much larger than the dose of morphine needed to produce antinociception when given with cannabinoids (Maguire et al., 2013; Maguire and France, 2014), might account for the differential development of tolerance across these studies. There was, however, another important difference between studies, which was the use of different approaches for monitoring the development of tolerance. In rats, changes in the effectiveness of a single dose were used to demonstrate that tolerance developed, whereas in monkeys, changes in potency were used, as determined by shifts in dose-effect curves, and this difference in the manner in which tolerance was shown precludes a direct comparison of the relative role of opioid treatment dose in this effect. Other studies in rodents used changes in potency to demonstrate an attenuation of morphine tolerance by concurrent cannabinoid administration, and in each case, the treatment dose of morphine was the same when given alone or in combination with a cannabinoid (Cichewicz and Welch, 2003; Fischer et al., 2010). Furthermore, in those studies using rodents, the dose of morphine administered daily was at least 3-fold larger than the dose needed to produce antinociceptive effects, whereas the treatment dose used in the current study was the smallest dose needed to produce the maximal latency in all four monkeys. Thus, differences in morphine treatment dose do not appear to account for these differences across studies.
Alternatively, the duration of the treatment period might impact whether morphine tolerance is attenuated or enhanced by cannabinoids. In each of the rodent studies in which tolerance was attenuated, the treatment period was 7 days, whereas in the current study in which tolerance was exacerbated, the treatment period was 80 days, and morphine dose-effect curves were determined multiple times during that treatment period. In monkeys receiving morphine alone, dose-effect curves were shifted to the right of the curve determined before chronic treatment and not further shifted between the first and last determinations during treatment [AUC (±1 S.E.M.): 15.22 ± 4.82 on day 13 compared with 12.57 ± 5.00 on day 55]; however, in monkeys receiving morphine and THC, the potency of morphine decreased markedly over the course of chronic treatment [AUC (±1 S.E.M.): 23.97 ± 2.08 on day 13 compared with 3.36 ± 1.11 on day 55]. Taken together, these data suggest that tolerance to combinations of opioids and cannabinoids might be greater with longer periods of treatment, indicating the need for additional studies to determine the effectiveness of this drug combination for treating chronic pain.
Although administering a cannabinoid concurrently with morphine enhanced the development of tolerance, it had little impact on the development of dependence, which was monitored by measuring physiologic withdrawal signs using telemetry and directly observable signs. Discontinuation of treatment with morphine alone increased daytime and nighttime heart rate, total score for directly observable withdrawal signs, and unusual tongue movement. These signs were reliably changed during opioid withdrawal in monkeys (Becker et al., 2008; Gerak et al., 2015) and were persistent, lingering for up to 1 month after treatment was discontinued. Discontinuation of treatment with a combination of morphine and THC also increased nighttime heart rate, total score for directly observable signs, and unusual tongue movement, and there was not a significant change in withdrawal signs that emerged after treatment with morphine given alone or together with THC. Although physiologic withdrawal signs were generally evident within 2 days of discontinuation of treatment with morphine alone, those same signs were not significantly changed until 5 days after discontinuation of treatment with the combination; the long duration of action of THC, and the possibility that it accumulated during chronic treatment, might have delayed or prevented the emergence of withdrawal signs (Ginsburg et al., 2014; Hruba and McMahon, 2014). Changes in heart rate tended to last longer after discontinuation of morphine alone, whereas directly observable signs were more persistent after termination of the combination. Despite minor but significant differences in withdrawal from the two treatment regimens, concurrent administration with THC did not exacerbate morphine withdrawal signs.
One strategy for reducing prevalence of prescription opioid abuse and overdose is to reduce the dose needed for pain relief. When combined with cannabinoids, smaller doses of opioids are needed for antinociception, thereby retaining the therapeutic effectiveness of opioids while reducing the likelihood of diversion and subsequent misuse. This approach would be less useful if adverse effects of opioids are also enhanced by cannabinoids. Although some effects of opioids are not changed or attenuated by cannabinoids, including discriminative stimulus and reinforcing effects along with dependence and withdrawal (current study; Li et al., 2008, 2012; Maguire et al., 2013), long-term treatment with large doses of the combination enhances opioid tolerance. The doses used in this study were larger than those that would be needed for pain relief; however, they were selected to determine whether cannabinoids exacerbate the development of tolerance to and dependence on a dose of morphine that produces tolerance and dependence when administered alone (Gerak et al., 2015). Current studies are exploring chronic treatment with smaller dose combinations of opioids and cannabinoids to see if tolerance develops to these small doses that are ineffective when given alone but effective in producing antinociceptive effects when given together.
Acknowledgments
The authors thank Charlene (Nicole) Garcia, Marlisa Jacobs, Andrew Lisenby, Carlos Moreno, Chris Robinson, and Crystal Taylor for expert technical assistance.
Authorship Contributions
Participated in research design: Gerak, France.
Conducted experiments: Gerak.
Performed data analysis: Gerak.
Wrote or contributed to the writing of the manuscript: Gerak, France.
Footnotes
- Received December 9, 2015.
- Accepted March 1, 2016.
This project was supported by the National Institutes of Health National Institute on Drug Abuse [Grants R01DA05018 and K05DA17918]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health.
Abbreviations
- ANOVA
- analysis of variance
- AUC
- area under the dose-effect curve
- CP 55,940
- 2-[(1R,2R,5R)-5-hydroxy-2-(3-hydroxypropyl) cyclohexyl]-5-(2-methyloctan-2-yl)phenol
- THC
- Δ9-tetrahydrocannabinol
- U-50,488
- trans-3,4-dichloro-N-methyl-N-[2-(1-pyrrolidinyl)-cyclohexyl]benzenacetamide methanesulfonate
- WIN 55,212
- (R)-(1)-[2,3-dihydro-5-methyl-3-(4-morpholinylmethyl)pyrrolo[1,2,3-de]-1,4-benzoxazin-6-yl]-1-naphthalenylmethanone mesylate
- Copyright © 2016 by The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}