


Abstract
The reinforcing effects of cocaine and methylphenidate have been linked to their ability to block dopamine transporters (DAT). Using positron emission tomography (PET), we previously showed that intravenous cocaine induced a significant level of DAT blockade, which was associated with the intensity for self-reports of “high” in cocaine abusers. In this study, we measured DAT occupancies after intravenous methylphenidate and assessed whether they also were associated with the “high”. Occupation of DAT by intravenous MP was measured with PET using [11C]cocaine, as a DAT ligand, in eight normal control subjects tested with different methylphenidate doses. The ratio of the distribution volume of [11C]cocaine in striatum to that in cerebellum, which corresponds toBmax/Kd + 1, was used as measure of DAT availability. In parallel, self-reports of “high” were measured. Methylphenidate produced a dose-dependent blockade of DAT with an estimated ED50 of 0.075 mg/kg. DAT occupancies were significantly correlated with the “high” (p < .03). However, four of the eight subjects, despite having significant levels of DAT blockade, did not perceive the “high”. Methylphenidate is as effective as cocaine in blocking DAT in the human brain (cocaine ED50 = 0.13 mg/kg), and DAT blockade, as for cocaine, was also associated with the “high”. However, the fact that there were subjects who despite significant DAT blockade did not experience the “high” suggests that DAT blockade, although necessary, is not sufficient to produce the “high”.
Methylphenidate (Ritalin) (MP), a drug used widely to treat children with attention deficit disorder (Carrey et al., 1996), blocks the dopamine transporters (DAT) (Ritz et al., 1987), which is an effect that has been linked to the reinforcing effects of cocaine as assessed by the good correlation between the affinity of drugs for the DAT and their reinforcing effects (Ritz et al., 1987). Methylphenidate (MP) has been shown to be self-administered by nonhuman primates in which it was shown to have equivalent reinforcing effects to those of cocaine (Johanson and Schuster, 1975; Bergman et al., 1989). When MP was administered intravenously to cocaine abusers, it induced a “high” that was reported to be almost indistinguishable from that induced by i.v. cocaine (Wang et al., 1997). MP has also been shown to be abused by humans, although its abuse is much less frequent than that of cocaine (NIDA-CEWG, 1995) and is predominantly restricted to the i.v. route of administration (Parran and Jasinski, 1991). Although the much less common use of MP than of cocaine could reflect market availability and drug trends, it also is possible that it reflects pharmacological differences between the two drugs, such as in vivo efficacy to block DAT and/or differences in pharmacokinetics (Volkow et al., 1995). Thus, the concern about the potential abuse liability of MP (Parran and Jasinski, 1991) emphasizes the need to understand better the variables affecting its reinforcing effects.
With positron emission tomography (PET) and appropriate radiotracers, it is now possible to measure reproducibly the levels of DAT occupancy achieved by drugs that block the DAT in human subjects (Volkow et al., 1997a). Using this strategy, we have shown a significant correlation between the magnitude of cocaine-induced DAT blockade and the self-reports for the “high” in cocaine abusers (Volkow et al., 1997a). It was of interest to determine whether we could replicate the correlation between DAT blockade and the “high” in normal control subjects tested with MP.
In this study, we used PET and [11C]cocaine as a DAT ligand (Fowler et al., 1989) to assess the level of DAT occupancy achieved with different doses of i.v. MP in human brain. The reinforcing effects of cocaine, which in humans are generally accompanied by self-reports of euphoria or “high” (Nestler, 1992), were assessed by asking participants to respond verbally to the self-reports of “high”. The self-reports for the “high” have been reported to be reliable and consistent across studies, and there is no other known measure that is better in predicting self-administration of drugs in humans (Fischman and Foltin, 1991). The results obtained with i.v. MP were compared with those we had previously reported for i.v. cocaine (Volkow et al., 1997a).
Materials and Methods
Subjects.
Eight healthy control subjects (five men and three women; age, 32 ± 7 years) were studied. Subjects with past and present histories of alcohol or drugs use (except for caffeine and cigarettes) were excluded from the studies. Prescan urinalysis ensured absence of psychoactive drug use. Subjects were instructed to discontinue any over-the-counter medication 1 week before the scan. Written informed consent was obtained in all subjects following the guidelines set by the Institutional Review Board at Brookhaven National Laboratory.
Scan.
PET studies were carried out with a Siemens CTI 931 tomograph (6 × 6 × 6.5-mm full-width half-maximum, 15 slices) using [11C]cocaine as a DAT ligand (Fowler et al., 1989). Methods for positioning and repositioning of subjects in the tomograph, alignment, arterial and venous catheterization, transmission scans, blood sampling, and blood analysis have been published (Fowler et al., 1989). Briefly, emission scans were started immediately after injection of 4 to 8 mCi of [11C]cocaine (specific activity > 0.2 Ci/μmol at time of injection). A series of 20 emission scans were obtained from time of injection up to 54 min. Arterial sampling was used to quantify total carbon-11 and unchanged [11C]cocaine in plasma as described (Fowler et al., 1989).
Each subject was scanned four times with [11C]cocaine over a 3-day period: one after placebo (baseline scan) and three times after different i.v. doses of MP (0.05, 0.1, 0.25, and 0.5 mg/kg). A different dose was used for each scan. The [11C]cocaine scans were performed 5 to 8 min after placebo (3 ml of saline) or 5 to 8 min after one of the MP doses. The placebo scan was done on the first day and was followed 2 h later by a second scan done after MP. On the 2nd and 3rd days of scanning, only one scan was performed using a different MP dose each day. Subjects were blind to the drug received, and the doses used were randomly assigned so that each dose was tested on six different subjects. Table 1 summarizes the doses of MP received by the subjects. The design of this study assumed that the intra- and intersubject variability in the DAT occupancy measures were equivalent. Venous blood was drawn for quantification of plasma concentration of MP before and at 27 and 47 min after MP using capillary GC/Mass spectrometry (Srinivas et al., 1991).
Doses of MP received by the different subjects
Behavioral Measures.
The subjective effects of MP were assessed by asking participants to orally respond to the following mood descriptors: “high”, “rush”, “anxious”, and “restless” every 5 min starting 15 min before placebo or MP, then every minute for 20 min, and then every 5 min for a total of 75 min. “High” was defined as euphoria, “rush” as the sensation of the drug in the body, and “restlessness” as the desire to move. To simulate an analog rating scale, participants were instructed to respond to each descriptor using a whole number between 0 (no effects) and 10 (maximal effects) (Wang et al., 1997). Effects of MP on heart rate and blood pressure were continuously monitored throughout the study.
Image Analyses.
Regions of interest in striatum and cerebellum were drawn directly on an averaged emission image (images obtained between 10 and 54 min) as previously described (Fowler et al., 1989). These regions were then projected into the dynamic images to generate time-activity curves for striatum and for cerebellum. These time-activity curves for tissue concentration along with the time-activity curves for unchanged tracer in plasma were used to calculate the distribution volume in striatum and cerebellum using the Logan Plot graphic analysis technique for reversible systems (Logan et al., 1990). The ratio of the distribution volume in striatum to that in cerebellum, which corresponds toBmax/Kd+ 1 and is insensitive to changes in cerebral blood flow, was our measure of DAT availability (Logan et al., 1994). DAT occupancies were calculated as [(Bmax/ Kdplacebo −Bmax/Kd MP)/Bmax/Kdplacebo] × 100.
Data Analyses.
Differences in DAT occupancy and in the behavioral and cardiovascular measures after placebo and after the different doses of MP were tested with ANOVA. For the behavioral measures, we averaged the scores obtained between 2 and 7 min after placebo or MP, and for the cardiovascular measures, we averaged the scores between 5 and 30 min because these were the time periods when peak effects for these measures occurred. Post hoc ttests then were performed to determine the doses for which the behavioral and cardiovascular effects were significant. Pearson’s product moment correlations analyses were calculated for the estimates of DAT occupancy and the behavioral and cardiovascular changes (MP − placebo) and between DAT occupancy and the concentration of MP in plasma.
To obtain the ED50 for MP (dose required to occupy 50% of DAT), the percent occupancy was linearized by plotting lnP/(100 − P) versus ln dose (mg/kg) whereP is the percent DAT occupancy; the linear regression enabled the determination of the ED50, which corresponds to the 0 value on the x-axis (Keen and MacDermot, 1993). The ED50 for MP was compared with the ED50 for cocaine, which was obtained using the previously published data on DAT occupancies for i.v. cocaine in cocaine abusers (Volkow et al., 1997a).
Results
MP decreased [11C]cocaine binding in striatum but not in cerebellum in a dose-dependent manner (Fig.1).Bmax/Kdmeasures were significantly reduced by all doses of MP, and the estimated DAT occupancies corresponded to 35 ± 5% for 0.025 mg/kg, 62 ± 13% for 0.1 mg/kg, 67 ± 3% for 0.25 mg/kg, and 78 ± 11% for 0.5 mg/kg (Fig.2A). The estimated ED50 (dose required to block 50% of the DAT) was 0.075 mg/kg (Fig. 2B). The estimated ED50 for i.v. cocaine calculated using previously published data was 0.13 mg/kg.

Distribution volume images of [11C]cocaine obtained at the level of the striatum (left) and the cerebellum (right) for one of the subjects tested at baseline (placebo) and with 0.025 and 0.1 mg/kg i.v. MP doses. MP dose-dependently decreased the binding of [11C]cocaine in striatum but not in cerebellum.

A, Relationship between DAT occupancy by MP and doses of MP (mg/kg). B, Linearized plots used to calculate the dose of MP required to occupy 50% DAT (dose ED50), which corresponded to 0.075 mg/kg (P = percent dopamine transporter occupancy).
The plasma concentration for MP is shown in Table2. DAT occupancies were significantly correlated with MP plasma concentration at 27 and 47 min after its administration (r = 0.72, df = 22,p < .0001) (Fig. 3).
Plasma concentration of MP at different times after its administration for the various doses

A, Correlation between DAT occupancy and plasma concentration of MP at 27 min after its administration. (r = 0.72, df = 22, p < .001). B, Correlation between DAT occupancy and plasma concentration of MP at 47 min (r = 0.72, df = 22,p < .001) after its administration.
MP significantly increased self-reports of “high” (F = 4.3, df = 4, 31, p < .008) and of “rush” (F = 3.2, df = 4, 31,p < .03), but its effects on anxiety or restlessness did not reach significance (Table 3). Post hoc t tests revealed that the effects on “high” and “rush” were significant for the 0.25 and 0.5 mg/kg doses. Self-reports of “high” and “rush” were significantly correlated with DAT blockade (r = 0.46, df = 23,p < .05) (Fig. 4). However, individual analysis of the data revealed that four of the eight subjects did not report a “high” after MP despite having DAT occupancies of greater than 60%.
Behavioral and cardiovascular measures after placebo or after the various MP doses

A, Relationship between DAT occupancy and self-report of “high” (r = 0.46, df = 23,p < .05). The numbers in the scattergram identify the subjects (see Table 1) who experienced a “high” and the subjects who did not experience a “high” but had DAT occupancies of >60%. B, Relationship between DAT occupancy and self-report of “rush” (r = 0.46, df = 23,p < .05).
MP induced a significant dose related increase in heart rate (F = 6.6, df = 4, 31, p < .0007), systolic (F = 4.9, df = 4, 31, p< .004), and diastolic blood pressure (F = 3.9, df = 4, 31, p < .01) (Table 2). Post hoct tests revealed that the effects on heart rate were significant for the 0.1, 0.25, and 0.5 mg/kg doses (p< .05), and for systolic and diastolic blood pressure, they were significant for the 0.25 and 0.5 mg/kg doses (p < .05). Levels of DAT blockade were significantly correlated with MP-induced (MP − placebo) increases in heart rate (r = 0.49, df = 23, p < .02) and in systolic blood pressure (r = 0.51, df = 23,p < .01) but not with diastolic blood pressure (r = 0.26, df = 23, p = 0.22) (Fig. 5).
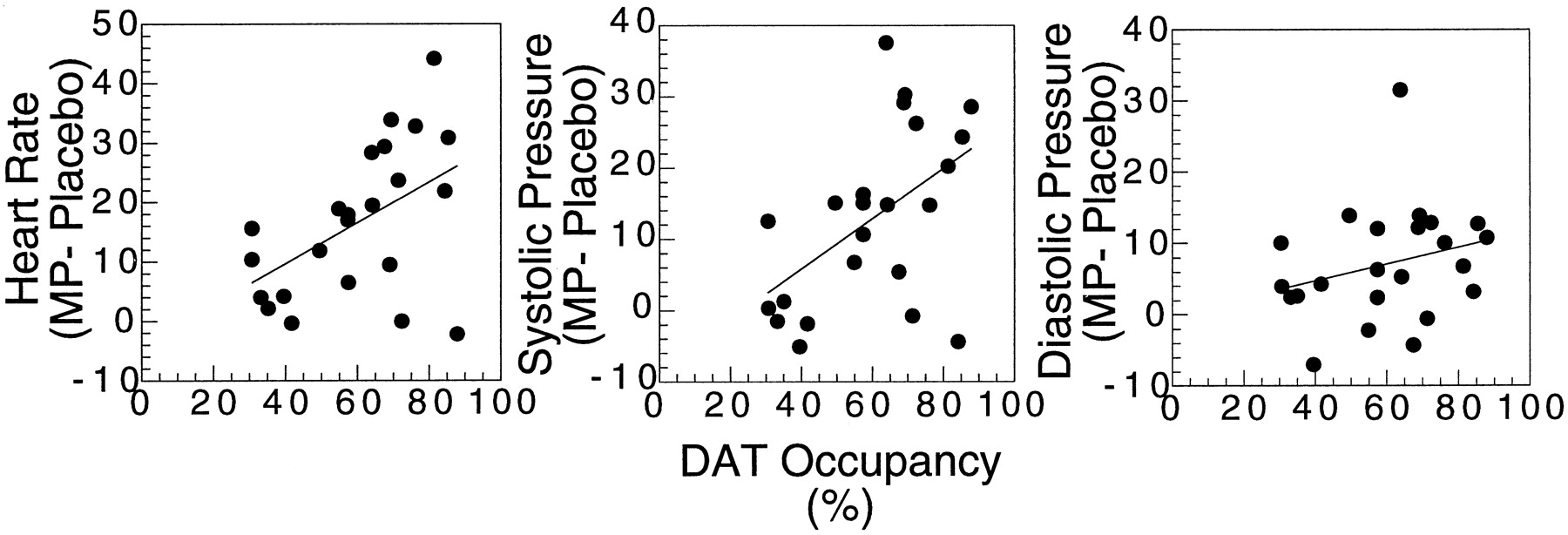
Relationship among DAT occupancy and MP-induced (MP − Placebo) increases in heart rate (r = 0.49, df = 23, p < .02), systolic blood pressure (r = 0.51, df = 23,p < .01), and diastolic blood pressure (r = 0.26, df = 23, p 0.22).
Discussion
These results corroborate an association between DAT occupancy and self-reports of “high” in non-drug-abusing subjects given i.v. MP. However, the correlation was weaker than that we had obtained for i.v. cocaine in cocaine abusers; in this study, DAT blockade accounted only for 21% of the variance, whereas in the study done in cocaine abusers, DAT blockade accounted for 31% (Volkow et al., 1997a). Moreover, with MP, only four of the eight subjects who showed DAT occupancies of greater than 60% reported a “high”, whereas all of the cocaine abusers in whom cocaine induced 60% blockade reported a “high”. The differences between the two studies could reflect differences in response to psychostimulant-induced “high” between controls and cocaine abusers and/or differences between MP and cocaine. Cocaine abusers may be sensitized to the “high” induced by cocaine and therefore may have been more likely to experience it after DAT blockade. Future studies evaluating the relation between the “high” and DAT blockade induced by MP in cocaine abusers will allow us to determine whether they are more sensitive to DAT blockade than controls. However, these results differ from those we had previously reported with a fixed dose of i.v. MP (0.5 mg/kg) in which we were unable to show a correlation between DAT blockade and the “high” in nonabusing control subjects (Volkow et al., 1996a). The range of DAT occupancies in that study was limited (70–83%) and that is why we believe we did not find an association with the “high”. In fact we also fail to observe a correlation between DAT blockade and “high” in the current study if we limit the analysis to the 71 to 87% range of DAT occupancies (r = 0.36, df = 6,p = .43). However, the failure to observe an association between DAT blockade and the “high” when the occupancies are limited to a very narrow range highlights the fact that variables other than DAT blockade are required to explain why in subjects with equivalent levels of DAT blockade, some experience the “high” and others do not.
Because DAT blockade by MP or by cocaine is the triggering event that leads to increases in synaptic DA and subsequent DA receptor stimulation, the variability could reflect these postsynaptic responses. In fact, blockade of D2 receptors decreases or abolishes the reinforcing effects of cocaine in laboratory animals (De Wit and Wise, 1977; Woolverton, 1986). Therefore, the variability in the response to MP among control subjects and the differences between the current study and the one in cocaine abusers could reflect in part differences in responses mediated by DA stimulation of D2 and/or D1receptors. That this may be the case is supported by studies showing that in control subjects, MP-induced changes in regional brain glucose metabolism are dependent in part on the availability of striatal D2 receptors (Volkow et al., 1997b). Furthermore, cocaine abusers, compared with control subjects, have fewer striatal D2 receptors (Volkow et al., 1990, 1993) and show a blunted response to MP-induced decreases in the binding of [11C]raclopride to D2receptors, a measure that reflects occupancy of D2 receptors by endogenous DA (Volkow et al., 1997c). Future studies evaluating the relation between MP-induced levels of D2 receptor occupancy by DA and the “high” will allow us to determine whether this is a better predictor of behavioral responses than levels of DAT blockade. The variability in the behavioral responses could also reflect differences in transduction responses (Nestler, 1992).
It is also possible that neurotransmitters other than DA may participate in the “high”. Cocaine, but not MP, blocks the serotonin transporter, and both drugs block the norepinephrine transporter (Gatley et al., 1996). The facts that i.v. MP has been shown to elicit a “high” similar to that of cocaine (Wang et al., 1997), that cocaine and MP show similar rates of self-administration in nonhuman primates (Johanson and Schuster, 1975; Bergman et al., 1989), and that MP substitutes for cocaine in discrimination studies (Wood and Emmett-Oglesby 1988) suggest that serotonin transporter blockade does not play a prominent role in the acute reinforcing effects of these drugs. However, chronic administration of cocaine may lead to different adaptation changes in the serotonin system than after chronic MP, which could affect the motivational drive for drug self-administration (Richardson and Roberts, 1991; Roberts et al., 1994), leading to differences in the addiction liability of these two drugs. The involvement of norepinephrine transporter blockade in the reinforcing effects of these two drugs is also unclear because although noradrenergic blockade does not affect cocaine self-administration (De Wit and Wise, 1977), it does affect its discriminative properties (Spealman, 1995; Kleven and Koek, 1997). Corelease of peptides and/or hormones such as cortisol could also modulate the reinforcing effects of cocaine and/or MP (Goeders, 1997). The contribution of variables other than DAT blockade in the reinforcing effects of cocaine are upheld by recent studies showing that DAT knockout mice self-administer cocaine and exhibit conditioned place preference (Rocha et al., 1998; Sora et al., 1998).
The differences in the ED50 between cocaine and MP (0.13 and 0.075 mg/kg, respectively) are compatible with differences in their affinities for DAT (Kifor inhibition of DA uptake correspond to 640 and 390 nM, respectively) (Ritz et al., 1987). The similar efficacy of MP and cocaine to block DAT in the human brain after their i.v. administration could explain the similar reinforcing effects reported for these two drugs (Johanson and Schuster, 1975; Bergman et al., 1989). Although to our knowledge no microdialysis study has compared DA changes induced by MP and by cocaine, review of separate studies indicates similar increases after their i.v. administration, that is, MP (2–10 mg/kg) increased DA 300 to 900% (Aoyama et al., 1996) and cocaine (1–2 mg/kg) 280 to 700% (Hurd and Ungerstedt, 1989; Moghaddam and Bunney, 1989). However, when comparing cocaine and MP, it is important to realize that MP is a racemic mixture—50% is an active enantiomer (d-threo-MP) and 50% is an inactive enantiomer (l-threo-MP) (Patrick et al., 1987), whereas cocaine is the enantiomerically pure (−)-cocaine. Thus, in this study, the DAT blockade is likely due tod-threo-MP because l-threo-MP shows no binding to DAT, nor does it increase DA (Ding et al., 1997). Future comparisons between cocaine and d-threo-MP may be more pertinent to the pharmacological characterization of these two drugs.
In analyzing the implications of the similar in vivo efficacy for DAT blockade by cocaine and MP, regarding the abuse potential of MP, it is important to emphasize that the similarities were observed after i.v. administration, which is not the route of administration used therapeutically. Because the rapidity of drug effects is an important variable in the reinforcing effects of drugs of abuse (Balster and Schuster, 1973), the results with i.v. MP, which leads to very fast uptake in brain, cannot be extrapolated to what happens when MP is taken orally, which results in a much slower brain uptake (Volkow et al., 1998). In fact, when given for therapeutic purposes, oral MP has not been associated with euphoric responses or with a “high” (Klein et al., 1997). Also, although cocaine and MP have similar efficacies at the DAT, they have different pharmacokinetics. In the human brain, the uptake of cocaine is slightly faster than that of MP (4–6 versus 8–10 min) and the rate of clearance is significantly faster for cocaine (20 min) than for MP (>90 min) (Volkow et al., 1995). Because we had shown that the “high” was associated only with the initial fast uptake of the drug in brain and not with its continuous presence, we have postulated that the slow clearance of MP from brain may interfere with its frequent repeated administration because it would lead to saturation of DAT (Volkow et al., 1995). Also, the longer half-life of MP than that of cocaine is likely to lead to more side effects, which may eventually interfere with its administration.
This study showed a correlation between DAT blockade and MP-induced changes in heart rate and in systolic but not in diastolic blood pressure. This association suggests that the cardiovascular effects of MP are in part mediated by central effects modulated by DA. This is in agreement with studies showing that the cardiovascular effects for stimulant drugs such as cocaine and amphetamine can be antagonized by administration of DA D2 receptor blockers (Tella, 1996). Failure to observe any correspondence between diastolic blood pressure and DAT blockade suggests that other factors, such as noradrenergic blockade, are involved in this response. We found a similar dissociation in a study that evaluated the temporal course of MP-induced cardiovascular changes, which showed that although the temporal course of the increases in heart rate and systolic pressure corresponded well with the pharmacokinetics of [11C]MP in striatum, those for diastolic blood pressure did not (Volkow et al., 1996b). However, it is also possible that the association between DAT blockade and changes in heart rate and systolic blood pressure reflect a spurious and not a causal association.
Limitations of this study include the inaccuracies posed by differences in nonspecific binding of [11C]cocaine between striatum and cerebellum and the use of the placebo scan as the measure that reflected no occupancy. The error introduced by differences in nonspecific binding between striatum and cerebellum has been estimated to be on the order of 10% (Volkow et al., 1995b), and that introduced by the competition of endogenous DA with [11C]cocaine for binding to the DAT has been estimated to be less than 5% (Gatley et al., 1995). Another limitation for the study is that measurements were made in the dorsal striatum and not in the nucleus accumbens, the structure in the striatum associated with drug reinforcement in laboratory animals (Pettit et al., 1984;Pontieri et al., 1996); however, DAT occupancy by MP should not differ appreciably between these brain regions (Izenwasser et al., 1990).
This study measures for the first time the levels of DAT blockade achieved after i.v. MP and shows that i.v. MP has a comparable efficacy to that of i.v. cocaine in blocking DAT in vivo in the human brain. This study also corroborates our previous findings in cocaine abusers of an association between DAT blockade and self-reports of “high” in controls subjects. However, the fact that there were subjects who despite significant DAT blockade did not experience the “high” after MP suggests that although DAT blockade may be necessary for the “high”, it is not sufficient, and additional factor or factors are required for the “high”.
Acknowledgments
We thank D. Schlyer and R. Carciello for Cyclotron operations; A. Levy and D. Warner for PET operations; C. Wong for data management; R. Ferrieri, C. Shea, R. MacGregor, and P. King for radiotracer preparation and analysis; P. Cerveny and N. Netusil for patient care; and T. Cooper for plasma analyses of MP.
Footnotes
-
Send reprint requests to: Nora D. Volkow, M.D., Medical Department, Build. 490, Brookhaven National Laboratory, Upton, NY 11973. E-mail: volkow{at}bnl.gov.
-
1 This research was carried out at Brookhaven National Laboratory under support by the U.S. Department of Energy Office of Health and Environmental Research under Contract DE-ACO2–98CH10886 and by the National Institute on Drug Abuse Grant DA09490–01.
- Abbreviations:
- MP
- methylphenidate
- DA
- dopamine
- DAT
- dopamine transporter
- PET
- positron emission tomography
- Received May 13, 1998.
- Accepted August 13, 1998.
- The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}