
Abstract
Our previous studies have shown that mangiferin decreased serum triglycerides and free fatty acids (FFAs) by increasing FFAs oxidation in both animal and cell experiments. This study sought to evaluate the effects of mangiferin on serum lipid profiles in overweight patients with hyperlipidemia. Overweight patients with hyperlipidemia (serum triglyceride ≥ 1.70 mmol/L and total cholesterol ≥ 5.2 mmol/L) were included in this double-blind randomized controlled trial. Participants were randomly allocated to groups, either receiving mangiferin (150 mg/day) or identical placebo for 12 weeks. The lipid profile and serum levels of mangiferin, glucose, L-carnitine, β-hydroxybutyrate and acetoacetate were determined at baseline and 12 weeks. A total of 97 participants completed the trial. Compared with the placebo control, mangiferin supplementation significantly decreased the serum levels of triglycerides and FFAs and insulin resistance index. Mangiferin supplementation also significantly increased the serum levels of mangiferin, high-density lipoprotein cholesterol, L-carnitine, β-hydroxybutyrate and acetoacetate and increased lipoprotein lipase activity. However, there were no differences in the serum levels of total cholesterol, low-density lipoprotein cholesterol, serum glucose and insulin between groups. Mangiferin supplementation could improve serum lipid profiles by reducing serum triglycerides and FFAs in overweight patients with hyperlipidemia, partly due to the promotion of FFAs oxidation.
Similar content being viewed by others


Introduction
Atherosclerosis and cardiovascular disease are the leading causes of death worldwide1,2. Hyperlipidemia and elevated free fatty acids (FFAs) are risk factors for these diseases1,3. An increase of 1 mmol/L in plasma triglyceride levels can lead to a 76% increase in cardiovascular disease risk in women and a 31% increase in men4. Elevated plasma triglycerides (TG) and FFA levels can increase the production of atherogenic chylomicron and very-low-density lipoprotein (VLDL) remnants, which can destroy vascular endothelial function and increase arterial stiffness. The possible mechanism of action of these effects is the activation of oxidative stress-responsive transcription factors, producing inflammatory cytokines and increasing the expression of adhesion molecules5,6. In addition, elevated plasma FFA can also lead directly to insulin resistance, which is strongly correlated with atherosclerosis and cardiovascular disease7. Therefore, lowering blood lipids, especially the levels of TG and FFAs, has been considered an effective strategy to reduce overall atherosclerosis and cardiovascular risk and it was included in The Adult Treatment Panel III8,9.
Different types of lipid-lowering drugs are widely used, many of which should be used long-term and have various adverse side effects, such as hepatotoxicity, renal toxicity and neurotoxicity10,11,12. However, it is still a challenge to develop more effective lipid-lowing drugs with fewer adverse side effects. Screening drugs from many phytochemicals may be a possible solution because most phytochemicals are currently considered to be less toxic and have numerous pharmacological functions.
Mangiferin, 1,3,6,7-tetrahydroxyxanthone-C2-β-D-glucoside, is a natural phytochemical present in various plants, including Anemarrhena asphodeloides, Mangifera indica and Mangifera persiciformis13. It has been shown that mangiferin has many beneficial biological activities, including anti-inflammatory, anti-oxidant and anti-diabetic effects14,15,16. Moreover, recent animal studies have shown that mangiferin may lower TG and total cholesterol (TC) levels in diabetic rats17,18. Furthermore, our laboratory has also confirmed that mangiferin had the effects of lowering TG and FFAs in hyperlipidemic hamsters, rats and hepG2 cell models, which may have been achieved by modulation of the key enzyme expression involved in inhibiting lipogenesis and promoting fatty acid oxidation in the liver19,20. However, the effect of mangiferin on blood lipids in overweight patients with hyperlipidemia remains unclear.
Based on the lipid-lowering effects of mangiferin in animal and cell experiments, we conducted this double-blind randomized clinical trial to evaluate the effects of mangiferin on blood lipid profiles in overweight patients with hyperlipidemia.
Results
Study participants
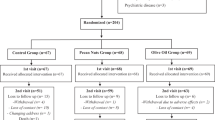
Among the 104 eligible individuals who participated in the study at baseline, 97 completed the trial and took all the tablets. Two individuals in the placebo group were excluded from the analysis because they changed their place of residence (n = 1) or did not take the suggested quantity of tablets (n = 1). Five individuals did not complete the study in the mangiferin supplementation group because they did not take the suggested quantity of tablets (n = 3) or were lost to follow-up (n = 2) (Fig. 1). There were no significant differences in the overall compliance rates between the two groups (P = 0.257).

Study design and the flow of participants.
Characteristics of the participants
At baseline, there were no significant differences between the placebo and mangiferin supplementation groups with respect to age, gender, body mass index (BMI) and blood pressure. There was also no difference in the lipid-lowering statin drugs taken between the two groups (Table 1). Dietary nutrient intakes in both groups did not differ significantly between the two groups at either baseline or the end of the intervention, suggesting that mangiferin did not suppress appetite at the dose used (Table 2).
Serum lipids, serum glucose and other metabolic variables
There were no significant differences in any variables between the two groups at baseline. After 12 weeks of the intervention, there was a significant increase in serum mangiferin levels and a significant decrease in serum TG and FFA levels in the mangiferin supplementation group compared with the control group. Furthermore, mangiferin significantly increased the levels of serum high-density lipoprotein (HDL), L-carnitine, β-hydroxybutyrate and acetoacetate levels. Although there were no differences in serum glucose and insulin levels between the control and mangiferin groups, mangiferin supplementation significantly decreased the insulin resistance index (HOMA-IR) compared with that of the placebo group. No significant changes in serum TC and low-density lipoprotein (LDL) levels were found after the end of the mangiferin intervention (Table 3).
Figure 2 shows the percentage differences in serum profiles between the mangiferin supplementation and placebo groups at the 12th week, adjusted for baseline values, serum mangiferin, age, gender, BMI, blood pressure, physical activity, hyperlipidemia duration and drug treatment determined by an analysis of covariance (ANCOVA). Compared with placebo, mangiferin supplementation significantly decreased the TG, FFA and HOMA-IR by 14.4%, 8.4% and 8.4%, respectively and increased serum mangiferin, HDL, LPL, L-carnitine, β-hydroxybutyrate and acetoacetate by 41.2%, 4.65%, 15.1%, 11.0%, 17.1% and 16.5%, respectively.

Differences between the mangiferin supplementation and placebo groups with respect to significant variables at the 12th week, adjusted for baseline values, serum mangiferin, age, gender, BMI, blood pressure, dietary intake, hyperlipidemia duration and drug treatment.
Serum FFA profile
Total serum fatty acids, total serum saturated fatty acids (SFA), total serum mono-unsaturated fatty acids (MUFA), total serum poly-unsaturated fatty acids (PUFA), total serum n-3 fatty acids and total serum n-6 fatty acids were significantly decreased in the mangiferin supplementation group compared with the controls. Further analysis of the serum FFA profiles showed that the contents of most fatty acids were also significantly decreased in the mangiferin supplementation group; only the contents of C14:0 and γ-C18:3 were not changed by mangiferin intervention (Table 4).
Hematologic measures and liver and kidney variables
Mangiferin supplementation had no significant effects on red blood cell, white blood cell and platelet counts or hemoglobin, total protein, albumin, urea nitrogen, creatinine, aspartate aminotransferase (AST) and alanine transaminase (ALT) levels compared with the control group (Table 5).
Discussion
This randomized, double-blind, placebo-controlled trial revealed that mangiferin supplementation for 12 weeks significantly decreased the serum TG, FFA and HOMA-IR levels and increased the serum mangiferin, HDL and LPL levels in overweight patients with hyperlipidemia. In addition, levels of L-carnitine, β-hydroxybutyrate and acetoacetate, which are used to diagnose fatty acid metabolism, were also increased by mangiferin. These results suggested that mangiferin supplementation could improve serum lipid profiles through the lowering of serum TG and FFA levels by promoting FFA oxidation.
Our previous study showed that one dose of oral mangiferin (900 mg) in humans did not produce any side effects or changes in clinical symptoms and blood biochemical variables21. As there have been no reports regarding mangiferin intervention for a long period of time in any human study, we selected a relatively low and safer dose of mangiferin (150 mg/d), which is 1/2 the 300 mg/d dose applied in rats. We reported that the lowest effective dose of mangiferin was 50 mg/kg body weight (BW) in rats19,20. The conversion coefficient from rats to humans is 6 according to the body surface area estimation method22. Therefore, the dose of 300 mg/d mangiferin in humans was calculated by 50 mg/kg BW * 6. In addition, we did not observe any side effects or changes in liver enzymes or kidney variables in the participants after the 12-week intervention.
Our previous studies showed that mangiferin could lower serum TG and FFA by regulating the key enzymes of FFA synthesis and oxidation in liver and muscle tissues in rats or HepG2 cells. This study aimed to investigate the effects of mangiferin on lowering serum TG and FFA in human intervention trials. The results showed that mangiferin supplementation significantly decreased serum TG levels in overweight patients with hyperlipidemia. The mechanism involved in lowering serum TG is either the inhibition of TG synthesis or acceleration of TG decomposition23,24,25 and the catabolism of TG was mainly investigated in this study. Serum TG is first hydrolyzed, which liberates FFA during TG catabolism26. Lipoprotein lipase (LPL) is the key enzyme that hydrolyzes circulating TG, delivering FFAs to peripheral tissues for utilization and storage27,28. In our study, serum TG was significantly decreased in the mangiferin supplementation group and serum LPL activity was significantly increased, which suggested that mangiferin at least partly increased TG hydrolysis by LPL and the decrease in serum TG was due to the increase in serum TG catabolism. In accordance with our findings, another recent animal study demonstrated that mangiferin could upregulate proteins important for mitochondrial bioenergetics and downregulate proteins controlling de novo lipogenesis, which could enable mangiferin to enhance energy expenditure and inhibit lipogenesis29. Apontes P et al. reported that mangiferin exerts its effects of lowering serum TG and improving glucose and insulin profiles by stimulating carbohydrate oxidation30.
Approximately 10% of serum FFAs are derived from the hydrolysis of serum TG and serum FFA levels should increase with the increase in TG hydrolysis31,32. However, the total FFA level was significantly decreased in the mangiferin supplementation group compared with the control group in our study. Furthermore, the effects of mangiferin supplementation on serum FFA profiles were observed in this study and the results showed that SFA, MUFA, PUFA, total serum n-3 fatty acids and total serum n-6 fatty acids in serum FFA profiles were significantly decreased in the mangiferin supplementation group and only C14:0 and γ-C18:3 had no statistically significant change after the intervention with mangiferin for 12 weeks. Therefore, we speculated that mangiferin decreased serum TG by the reduction of serum total FFA. However, there was no significant effect of mangiferin supplementation on the chain lengths and degree of unsaturation of FFA.
The major organ for FFA metabolism is the liver at rest and the muscle during activity33. FFA enters these organs, where it can either be oxidized in the mitochondria to form ATP or esterified to produce TG for storage or incorporation into VLDL particles34. L-carnitine and carnitine palmitoyltransferase (CPT) are essential for the translocation of long-chain fatty acids that have entered the mitochondria and their quantities have been used for the testing of fatty acid metabolism35. Serum L-carnitine levels increase when β-oxidation rates are in excess of the rate of complete oxidation to CO2 through the tricarboxylic acid (TCA) cycle36,37. In our study, the serum L-carnitine level was significantly increased after mangiferin supplementation for 12 weeks, which indicated that mangiferin increased FFA oxidation by promoting the movement of FFA into mitochondria for oxidation by the carnitine carrier.
β-Hydroxybutyrate and acetoacetate may also help us to understand the above data. β-Hydroxybutyrate and acetoacetate (ketone body) are the main alternative energy substrates to glucose and they are mainly generated by the oxidation of FFA that are transported into the blood and utilized as a fuel for other cells; therefore, they should also be elevated in parallel with the increase in FFA oxidation38,39,40. However, β-hydroxybutyrate and acetoacetate were significantly increased in the mangiferin supplementation group in our study. In addition, we demonstrated that mangiferin could increase serum β-hydroxybutyrate in hyperlipidemic rats20. Therefore, we concluded that the increased β-hydroxybutyrate and acetoacetate levels induced by mangiferin may have originated from the increase in FFA oxidation in the mitochondria.
In conclusion, our results suggest that mangiferin can decrease the levels of serum TG and FFAs. It can also promote FFA oxidation by increasing serum L-carnitine, β-hydroxybutyrate and acetoacetate levels in overweight patients with hyperlipidemia. However, further studies are needed to evaluate and quantify the rate of FFA oxidation in overweight patients with hyperlipidemia treated by mangiferin.
Methods
Participants
Study participants with established hyperlipidemia were recruited from five communities in Harbin, China. The primary selection criteria included the following: age between 35 and 65 years; BMI ≥ 24.0; no cardiovascular disease, diabetes mellitus, or liver/renal disease; and a history of hyperlipidemia based on a print-out dated within half a year showing a plasma TG concentration ≥ 1.70 mmol/L and plasma TC concentration ≥ 5.20 mmol/L. Participants were excluded if they had taken traditional Chinese medicine or lipid-lowing drugs, except for statins. Based on the examination of 387 overweight subjects, we recruited a total of 104 eligible overweight patients with hyperlipidemia who agreed to participate in this study. All participants provided written informed consent to participate in this study, which was approved by the Human Ethics Committee of the Harbin Medical University.
Mangiferin intervention
Before the study was conducted, we treated rats and hamsters with mangiferin for 6 weeks. We observed significant decreases in blood lipid levels caused by mangiferin. We selected a relatively lower and safer dose of mangiferin (150 mg/d) for the study participants, which was 1/2 the dose of 300 mg/d used in our previous animal studies19 and was calculated based on the specific surface area according to the weight of the average human (60 kg). Mangiferin powder (purity 98%) was purchased (Xi An, China) and extracted from Anemarrhena asphodeloides Bunge. Mangiferin was incorporated into tablets using maize starch by Harbin Pharmaceutical Group 6th Pharm Factory, with each tablet containing 150 mg mangiferin. An identical placebo was produced, which contained only maize starch. Participants were asked to take 1 tablet each day.
Study design
This 12-week, double-blind, placebo-controlled study was registered at Current Controlled Trials (http://www.chictr.org, registration number: ChiCTR-TRC-13003962). The participants were stratified by serum TG levels and randomly assigned to take either placebo or mangiferin (150 mg/d). Participants were instructed not to change their usual diets, physical activity levels, or medications throughout the study. The participants were assigned to either supplement A or B according to a computer-generated blocked randomization schedule. The study coordinator assigned the participants to the supplement specified by the schedule in chronological order as the participants enrolled. Assignment into each study group remained concealed until participant enrollment was completed. A safety monitor who was otherwise uninvolved with the study held the key to the blinded assignments in a sealed envelope until all results were obtained and analyzed.
Compliance of the study participants was assessed by conducting scheduled telephone interviews and by counting the remaining tablets every two weeks. The study was approved by the ethics committee of Harbin Medical University and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Demographic characteristics
Demographic data were collected at baseline using a standardized questionnaire. Information collected included age, gender, physical activity, current smoking habits, hyperlipidemia duration and medications. Physical activity level was assessed using a physical activity questionnaire and calculated using a formula from the American Institute of Medicine41. At baseline and the 12th week, dietary intakes were measured with a validated semi-quantitative food-frequency questionnaire (FFQ). Energy and nutrient intakes were calculated using the Food Nutrition Calculator (V1.60; Shixinghengxun, Beijing, China).
Anthropometric and blood chemistry measurements
Anthropometric indices were measured by well-trained examiners with participants wearing light, thin clothing and no shoes. Body weight and height were measured to the nearest 0.1 kg and 0.1 cm, respectively. All participants were instructed to fast for 10 h and fasting venous blood samples were collected from the elbow in the morning both at baseline and at 12 weeks. Serum mangiferin was determined by high-performance liquid chromatography-mass spectrometry (HPLC-MS) according to our established method21. Serum TC, TG, HDL, LDL, glucose, β-hydroxybutyrate, acetoacetate, AST, ALT, total protein, albumin and blood urea nitrogen (BUN) were determined using a ROCHE Modular P800 Automatic Biochemical Analyzer (Roche Diagnostics, Mannheim, Germany). Serum insulin concentration was measured by a ROCHE Elecsys 2010 Chemiluminescence Immune Analyzer (Roche Diagnostics). Serum carnitine level was determined by enzymatic colorimetric methods with commercial kits (Bangjing, Shanghai, China). Serum LPL concentration was measured by an enzyme-linked immunosorbent assay (ELISA) using commercially available ELISA Kits (R&D System, USA). Serum FFA were determined by Gas Chromatography-Mass Spectrometer (TRACE GC/PolarisQ MS, Thermo Finnigan, USA) as described previously by our laboratory42. The blood cell count and hemoglobin concentration were determined using a SYSMEX-SF-3000 Automatic Hematology Analyzer (Sysmex Corporation, Kobe, Japan). The insulin resistance index (HOMA-IR) was calculated using the following formula: fasting insulin (μU/ml) × fasting blood glucose (mmol/l) / 22.543.
Statistical analysis
Data are presented as the mean ± SD or percentage. The χ2 test was used to compare categorical variables. Mean levels of continuous study variables at baseline and the 12th week were compared between the two groups by an analysis of covariance (ANCOVA). Paired-samples t tests were used to evaluate the changes in outcome variables before and after the intervention in each group. The ANCOVA was adjusted for baseline values of serum mangiferin, age, gender, BMI, blood pressure, dietary intake, hyperlipidemia duration and drug treatment. The percentage differences between the mangiferin and placebo groups in outcome variables were calculated using covariate-adjusted values, such as 100 × (treatment group-placebo group)/placebo group, for each study variable. Statistical analyses were carried out using SPSS (version 13.01S, Beijing Stats Data Mining Co. Ltd, Beijing, China). All P values were two-tailed and P < 0.05 was considered to indicate statistical significance.
Additional Information
How to cite this article: Na, L. et al. Mangiferin supplementation improves serum lipid profiles in overweight patients with hyperlipidemia: a double-blind randomized controlled trial. Sci. Rep. 5, 10344; doi: 10.1038/srep10344 (2015).
References
Lucchi, T. & Vergani, C. [Dyslipidemias and statins: from guidelines to clinical practice. An updated review of the literature]. G Ital Cardiol (Rome). 15, 149–60 (2014).
Yin, K. & Tang, C. Inflammation, lipid metabolism dysfunction and hypertension: active research fields in atherosclerosis-related cardiovascular disease in China. Sci China Life Sci. 54, 976–9 (2011).
Nordestgaard, B.G. & Varbo, A. Triglycerides and cardiovascular disease. Lancet. 384, 626–35 (2014).
Austin, M.A. Epidemiology of hypertriglyceridemia and cardiovascular disease. Am J Cardiol. 83, 13F–16F (1999).
Matsumoto, S., et al. The role of hypertriglyceridemia in the development of atherosclerosis and endothelial dysfunction. Nutrients. 6, 1236–50 (2014).
Pirro, M., et al. Plasma free fatty acid levels and the risk of ischemic heart disease in men: prospective results from the Quebec Cardiovascular Study. Atherosclerosis. 160, 377–84 (2002).
Frohnert, B.I., et al. Relation between serum free fatty acids and adiposity, insulin resistance and cardiovascular risk factors from adolescence to adulthood. Diabetes. 62, 3163–9 (2013).
Brewer, H.B., Jr. New features of the National Cholesterol Education Program Adult Treatment Panel III lipid-lowering guidelines. Clin. Cardiol. 26, III19–24 (2003).
Preiss, D. & Sattar, N. Lipids, lipid modifying agents and cardiovascular risk: a review of the evidence. Clin. Endocrinol. (Oxf). 70, 815–28 (2009).
Wlotzke, U., Hohenleutner, U., Abd-El-Raheem, T.A., Baumler, W. & Landthaler, M. Side-effects and complications of flashlamp-pumped pulsed dye laser therapy of port-wine stains. A prospective study. Br. J. Dermatol. 134, 475–80 (1996).
Kiortsis, D.N., Nikas, S., Hatzidimou, K., Tsianos, E. & Elisaf, M.S. Lipid-lowering drugs and serum liver enzymes: the effects of body weight and baseline enzyme levels. Fundam Clin. Pharmacol. 17, 491–4 (2003).
Muscari, A., Puddu, G.M. & Puddu, P. Lipid-lowering drugs: are adverse effects predictable and reversible? Cardiology. 97, 115–21 (2002).
Matkowski, A., Kus, P., Goralska, E. & Wozniak, D. Mangiferin - a bioactive xanthonoid, not only from mango and not just antioxidant. Mini Rev. Med. Chem. 13, 439–55 (2013).
Gong, X., et al. Anti-inflammatory effects of mangiferin on sepsis-induced lung injury in mice via up-regulation of heme oxygenase-1. J. Nutr. Biochem. 24, 1173–81 (2013).
Prabhu, S., Jainu, M., Sabitha, K.E. & Devi, C.S. Role of mangiferin on biochemical alterations and antioxidant status in isoproterenol-induced myocardial infarction in rats. J. Ethnopharmacol. 107, 126–33 (2006).
Sellamuthu, P.S., Arulselvan, P., Fakurazi, S. & Kandasamy, M. Beneficial effects of mangiferin isolated from Salacia chinensis on biochemical and hematological parameters in rats with streptozotocin-induced diabetes. Pak J. Pharm. Sci. 27, 161–7 (2014).
Rodriguez, J., et al. Effects of a natural extract from Mangifera indica L and its active compound, mangiferin, on energy state and lipid peroxidation of red blood cells. Biochim. Biophys. Acta. 1760, 1333–42 (2006).
Miura, T., et al. The suppressive effect of mangiferin with exercise on blood lipids in type 2 diabetes. Biol. Pharm. Bull. 24, 1091–2 (2001).
Guo, F., et al. Beneficial effects of mangiferin on hyperlipidemia in high-fat-fed hamsters. Mol. Nutr. Food Res. 55, 1809–18 (2011).
Niu, Y., et al. Mangiferin decreases plasma free fatty acids through promoting its catabolism in liver by activation of AMPK. PLoS One. 7, e30782 (2012).
Hou, S., et al. Pharmacokinetic study of mangiferin in human plasma after oral administration. Food Chem. 132, 289–94 (2012).
Lam, T.K. & Leung, D.T. More on simplified calculation of body-surface area. N Engl. J. Med. 318, 1130 (1988).
Rodriguez, M., et al. Plasma fatty acids and [13C]linoleic acid metabolism in preterm infants fed a formula with medium-chain triglycerides. J. Lipid Res. 44, 41–8 (2003).
Bjorntorp, P. Liver triglycerides and metabolism. Int. J. Obes. Relat. Metab. Disord. 19, 839–40 (1995).
Volek, J.S., et al. Effects of a high-fat diet on postabsorptive and postprandial testosterone responses to a fat-rich meal. Metabolism. 50, 1351–5 (2001).
Ringseis, R. & Eder, K. Regulation of genes involved in lipid metabolism by dietary oxidized fat. Mol. Nutr. Food Res. 55, 109–21 (2011).
Franssen, R., Monajemi, H., Stroes, E.S. & Kastelein, J.J. Obesity and dyslipidemia. Med. Clin. North. Am. 95, 893–902 (2011).
Brautbar, A., et al. LPL gene variants affect apoC-III response to combination therapy of statins and fenofibric acid in a randomized clinical trial of individuals with mixed dyslipidemia. J Lipid Res. 53, 556–60 (2012).
Lim, J., et al. Dual mode action of mangiferin in mouse liver under high fat diet. PLoS One. 9, e90137 (2014).
Apontes, P., et al. Mangiferin stimulates carbohydrate oxidation and protects against metabolic disorders induced by high-fat diets. Diabetes. 63, 3626–36 (2014).
Nielsen, S. & Karpe, F. Determinants of VLDL-triglycerides production. Curr. Opin. Lipidol. 23, 321–6 (2012).
Ebbert, J.O. & Jensen, M.D. Fat depots, free fatty acids and dyslipidemia. Nutrients. 5, 498–508 (2013).
Votruba, S.B. & Jensen, M.D. Regional fat deposition as a factor in FFA metabolism. Annu. Rev. Nutr. 27, 149–63 (2007).
Teusink, B., et al. Contribution of fatty acids released from lipolysis of plasma triglycerides to total plasma fatty acid flux and tissue-specific fatty acid uptake. Diabetes. 52, 614–20 (2003).
Stephens, F.B. & Galloway, S.D. Carnitine and fat oxidation. Nestle Nutr. Inst. Workshop Ser. 76, 13–23 (2013).
Wutzke, K.D. & Lorenz, H. The effect of l-carnitine on fat oxidation, protein turnover and body composition in slightly overweight subjects. Metabolism. 53, 1002–6 (2004).
Ramos-Roman, M.A., Sweetman, L., Valdez, M.J. & Parks, E.J. Postprandial changes in plasma acylcarnitine concentrations as markers of fatty acid flux in overweight and obesity. Metabolism. 61, 202–12 (2012).
Fukao, T., et al. Ketone body metabolism and its defects. J. Inherit. Metab. Dis. 37, 541–51 (2014).
Plourde, M., Tremblay-Mercier, J., Fortier, M., Pifferi, F. & Cunnane, S.C. Eicosapentaenoic acid decreases postprandial beta-hydroxybutyrate and free fatty acid responses in healthy young and elderly. Nutrition. 25, 289–94 (2009).
Keller, U., Gerber, P.P. & Stauffacher, W. Fatty acid-independent inhibition of hepatic ketone body production by insulin in humans. Am. J. Physiol. 254, E694–9 (1988).
Trumbo, P., Schlicker, S., Yates, A.A. & Poos, M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc. 102, 1621–30 (2002).
Liu, L., et al. Free fatty acid metabolic profile and biomarkers of isolated post-challenge diabetes and type 2 diabetes mellitus based on GC-MS and multivariate statistical analysis. J. Chromatogr B Analyt Technol. Biomed Life Sci. 878, 2817–25 (2010).
Moro, E., et al. Hypertriglyceridemia is associated with increased insulin resistance in subjects with normal glucose tolerance: evaluation in a large cohort of subjects assessed with the 1999 World Health Organization criteria for the classification of diabetes. Metabolism. 52, 616–9 (2003 ).
Acknowledgements
This study was supported by grants from the China Postdoctoral Science Foundation funded project (2014T70372, 2013M541415), the National Natural Science Foundation of China (81130049, 81372997), the Heilongjiang Postdoctoral Science Foundation (LBH-Z12163), the Research Fund for Innovation Talents of Science and Technology in Harbin City (No. 2012RFQXS080) and Wu Liande Grant of Harbin Medical University (WLD-QN1406).
Author information
Authors and Affiliations
Contributions
LX.N., Q.Z., Y.L., CH.S. and YC.N. conceived and designed the experiments. Q.Z., S.J., SS.D. and W.Z. performed the experiments and analyzed the data. LX.N. and YC.N. wrote the main manuscript text. Q.Z. and S.J. prepared all figures and tables. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Na, L., Zhang, Q., Jiang, S. et al. Mangiferin supplementation improves serum lipid profiles in overweight patients with hyperlipidemia: a double-blind randomized controlled trial. Sci Rep 5, 10344 (2015). https://doi.org/10.1038/srep10344
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep10344
This article is cited by
-
Combination of mangiferin and T0901317 targeting autophagy promotes cholesterol efflux from macrophage foam cell in atherosclerosis
Chinese Medicine (2024)
-
Pharmacological properties of mangiferin: bioavailability, mechanisms of action and clinical perspectives
Naunyn-Schmiedeberg's Archives of Pharmacology (2024)
-
Phospholipid complex-loaded self-assembled phytosomal soft nanoparticles: evidence of enhanced solubility, dissolution rate, ex vivo permeability, oral bioavailability, and antioxidant potential of mangiferin
Drug Delivery and Translational Research (2021)
-
Xiao Ke Qing improves glycometabolism and ameliorates insulin resistance by regulating the PI3K/Akt pathway in KKAy mice
Frontiers of Medicine (2018)
-
Mangiferin suppresses endoplasmic reticulum stress in perivascular adipose tissue and prevents insulin resistance in the endothelium
European Journal of Nutrition (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
