
Abstract
Introduction
Cannabinoids produce a spectrum of effects in humans including euphoria, cognitive impairments, psychotomimetic effects, and perceptual alterations. The extent to which dopaminergic systems contribute to the effects of Δ-9-tetrahydrocannabinol (Δ-9-THC) remains unclear. This study evaluated whether pretreatment with a dopamine receptor antagonist altered the effects of Δ-9-THC in humans.
Materials and methods
In a 2-test-day double-blind study, 28 subjects including healthy subjects (n = 17) and frequent users of cannabis (n = 11) were administered active (0.057 mg/kg) or placebo oral haloperidol in random order followed 90 and 215 min later by fixed order intravenous administration of placebo (vehicle) and active (0.0286 mg/kg) Δ-9-THC, respectively.
Results
Consistent with previous reports, intravenous Δ-9-THC produced psychotomimetic effects, perceptual alterations, and subjective effects including “high.” Δ-9-THC also impaired verbal recall and attention. Haloperidol pretreatment did not reduce any of the behavioral effects of Δ-9-THC. Haloperidol worsened the immediate free and delayed free and cued recall deficits produced by Δ-9-THC. Haloperidol and Δ-9-THC worsened distractibility and vigilance. Neither drug impaired performance on a motor screening task, the Stockings of Cambridge task, or the delayed match to sample task. Frequent users had lower baseline plasma prolactin levels and blunted Δ-9-THC induced memory impairments.
Conclusions
The deleterious effects of haloperidol pretreatment on the cognitive effects of Δ-9-THC are consistent with the preclinical literature in suggesting crosstalk between DAergic and CBergic systems. However, it is unlikely that DA D2 receptor mechanisms play a major role in mediating the psychotomimetic and perceptual altering effects of Δ-9-THC. Further investigation is warranted to understand the basis of the psychotomimetic effects of Δ-9-THC and to better understand the crosstalk between DAergic and CBergic systems.
Similar content being viewed by others


Introduction
Cannabis is one of the most widely used illicit substances (Compton et al. 2004; SAMHSA 2004). The primary active cannabinoid in cannabis is Δ-9-tetrahydrocannabinol (Δ-9-THC), but cannabis also contains more than 60 other cannabinoids, some of which may contribute either directly or indirectly to the effects of Δ-9-THC. The spectrum of effects produced by cannabis includes euphoria, relaxation, anxiety, perceptual alterations, paranoia, and impairments in attention and memory. Laboratory experiments have demonstrated that synthetic and natural cannabinoids can induce transient psychotomimetic effects in healthy human subjects (D’Souza et al. 2004; Henquet et al. 2006; Leweke et al. 1999) and exacerbate psychosis in individuals with schizophrenia (D’Souza et al. 2005). Finally, a growing body of epidemiological studies (reviewed in Fergusson et al. 2006; Henquet et al. 2005) have drawn attention to the link between cannabinoids and psychosis (D’Souza 2007).
Converging preclinical evidence suggests interactions between cannabinoid (CB1) and dopamine (DA) systems (reviewed in Gardner 2005; Laviolette and Grace 2006a). CB1 and D2 receptors are coexpressed in several brain regions (Hermann et al. 2002), and there is signal transduction convergence in these regions (Meschler and Howlett 2001). Δ-9-THC activates DAergic mesolimbic neurons (French 1997; French et al. 1997; Gardner 2005; Gessa et al. 1998) and induces DA release in the striatum (Chen et al. 1990a; Tanda et al. 1997a) in animals. CB1 agonists induce c-fos in the nucleus accumbens (Miyamoto et al. 1996) and A10 DArgic neurons within the ventral tegmentum (Patel and Hillard 2003). At a molecular level, DA D2 receptors are believed to have a significant modulatory role in determining the G-protein coupling specificity of CB1 receptors (Jarrahian et al. 2004). Haloperidol and Δ-9-THC produce more catalepsy in rats than haloperidol alone (Marchese et al. 2003), haloperidol reverses Δ-9-THC reductions in prepulse inhibition and startle response in mice (Nagai et al. 2006); however, haloperidol has no influence on Δ-9-THC-induced catalepsy in mice (Kinoshita et al. 1994). Given the preclinical evidence of crosstalk between CB and DA systems, one logical question is to what extent, if any, are DA receptor mechanisms involved in the psychotomimetic and rewarding effects of cannabinoids in humans?
Haloperidol was hypothesized to reduce the psychotomimetic, perceptual altering, euphoric, and cognitive effects of Δ-9-THC in humans and that the two drugs would have additive cataleptic effects. Further, there are long-term changes associated with exposure to cannabinoids (reviewed in D’Souza et al. 2008: In review; Kolb et al. 2006; Lichtman and Martin 2005; Ranganathan et al. 2007), including regional changes in DA transmission (Jentsch et al. 1998; Verrico et al. 2003). Therefore, individuals who frequently used cannabis were hypothesized to differ in their response to the interactive effects of haloperidol and Δ-9-THC.
Materials and methods
The study was conducted at the Neurobiological Studies Unit (VA Connecticut Healthcare System, West Haven, CT) with the approval of the Institutional Review Boards of VA Connecticut Healthcare System and Yale University School of Medicine and in accordance with the Helsinki Declaration of 1975. Subjects were informed about the side effects of both haloperidol (sedation, akathisia, dystonia, etc.) and Δ-9-THC (euphoria, anxiety, paranoia, etc.). Subjects were recruited by public advertisement and compensated for their research participation. Confidentiality of study data was protected.
Participants
The sample consisted of two groups, frequent users of cannabis and healthy subjects. Frequent users were defined as (1) lifetime cannabis exposure greater than or equal to 100 times, (2) last exposure to cannabis within the past week, (3) recent cannabis exposure greater than ten times per month as quantified by Time Line Follow Back (Sobell and Sobell 1992), and (4) positive urine toxicological test for cannabis at screening. These subjects also met criteria for Diagnostic and Statistical Manual of Mental Disorders (DSM) IV cannabis abuse disorder, while none of the healthy subjects did.
In addition to obtaining written informed consent, subjects had to successfully complete a questionnaire about the key risks and benefits of the study. Subjects (18–55 years) underwent a structured psychiatric interview for DSM (First et al. 2002; Spitzer 1990) and were carefully screened for any DSM axes I or II lifetime psychiatric or substance use disorder (except for cannabis in the case of frequent users) and family history of major axis I disorder. All subjects were asked to estimate their lifetime cannabis exposure (number of times), heaviest exposure, and last exposure to cannabis. Subjects were excluded for recent abuse (3 months) or dependence (1 year) to alcohol or any substances, other than nicotine in both groups. Cannabis-naïve individuals were excluded to minimize any risk of promoting future cannabis use/abuse. The history provided by subjects was confirmed by a telephone interview conducted with an individual (spouse or family member) identified by the subject before screening. A general physical and neurological examination, electrocardiogram, and laboratory tests (serum electrolytes, liver function tests, complete blood count with differential, and urine toxicology) were also conducted. Subjects were instructed to refrain from alcohol, illicit drugs, or prescription drugs not approved by the research team for 2 weeks before the study and throughout study participation. Healthy subjects were required to have a negative urine toxicological test at screening. Frequent users were permitted to use cannabis until 24 h before each test day, to minimize cannabis withdrawal, a syndrome that has been described by several groups (Budney et al. 2003; Haney 2005; Haney et al. 1999a, b). Abstinence from cannabis in the 24 h before each test day was confirmed by subject interview on each test day. Self-reported cannabis use is a valid method of assessing cannabis use (Martin et al. 1988).
Experimental design
Subjects completed 2 test days during which they received placebo or active (0.057 mg/kg) haloperidol in random counterbalanced order, followed 90 min later by placebo Δ-9-THC (vehicle) and 215 min later by active Δ-9-THC (0.0286 mg/kg) administered intravenously (i.v.) over 20 min in a fixed order (Table 1).
Drugs
The dose and rate of administration of Δ-9-THC was chosen to mimic the dose range of recreational cannabis use and to be equivalent to about 0.5–1.5 of a standard National Institute of Drug Abuse cannabis cigarette. Further, in pilot studies, because subjects were unable to tolerate higher doses, Δ-9-THC (0.05, 0.035 mg/kg) was given as a 2-min bolus after receiving haloperidol. A 20-min infusion was selected to mimic the time frame of recreational cannabis consumption. The rationale for the route of Δ-9-THC administration and preparation of both Δ-9-THC and placebo is described previously (D’Souza et al. 2004, 2005). The psychoactive effects of cannabis in humans are due primarily to Δ-9-THC (Wachtel et al. 2002). Δ-9-THC of 99.6% purity was dissolved in 95% ethanol (Agurell et al. 1986) to yield a concentration of 2 mg/ml stock solution, which was then passed through a 0.22 μm polymer filter, subjected to sterility and pyrogenicity testing, assayed by gas chromatography–mass spectrometry to confirm its concentration, and stored at −20°C for future use. For the control condition, an equivalent volume (≅x2 ml) of ethanol (vehicle) was used, which would amount to a concentration of 0.0004% in an adult with average blood volume (4–5 l). Postinjection blood sampling at multiple time points failed to detect ethanol.
The DA receptor antagonist haloperidol was chosen because of its relative specificity for D2 receptors. In pilot studies, 0.05 mg/kg haloperidol (3.5 mg in a 70 kg individual) produced no appreciable effects, while at 0.071 mg/kg (5 mg in a 70 kg individual), it was associated with a high rate of dropouts related to side effects (D’Souza, unpublished observations). Therefore, an intermediate dose of haloperidol (0.057 mg/kg), equivalent to 4 mg in a 70-kg individual, was chosen. This dose was expected to produce antipsychotic effects without producing significant extrapyramidal side effects (Farde et al. 1992; Kapur et al. 1997, 2000) and is within the dose range recommended by the British Association of Psychopharmacology consensus conference for the use of haloperidol in healthy volunteers (King 1997). Further, at this dose, haloperidol is a relatively selective antagonist at DA D2 receptors (Schotte et al. 1996) compared to actions at other receptors (e.g., muscarinic M1 or histaminergic H1) that might modulate Δ-9-THC effects.
Test days were separated by at least 1 week (greater than three times the elimination half life of Δ-9-THC) to minimize carryover effects (Wall et al. 1976). To keep both subjects and raters blind to study conditions and the order of drug administration, both the subjects and raters were told of a possibility of a third “very low” dose of both haloperidol and Δ-9-THC, deliberately described in ambiguous terms. In actuality, subjects never received the “very low” dose of both haloperidol and Δ-9-THC.
Schedule of testing
Urine toxicology was conducted on the morning of each test day to rule out recent illicit drug use. A positive urine drug screen resulted in exclusion from the study except when positive for cannabis in frequent users. Subjects fasted overnight, reported to the test facility around 8 a.m., and were provided a standard breakfast. A positive urine pregnancy test also resulted in exclusion.
The detailed schedule of test procedures is described in Table 1. Subjects were attended to by a research psychiatrist, a research nurse, and a research coordinator. Clear “stopping rules” were determined a priori, and rescue medications were available during testing (lorazepam and benztropine) if necessary and also at discharge (diphenhydramine). Subjects were recontacted at 1, 3, and 6 months post-study for safety follow-up.
Outcome measures
Behavioral and subjective ratings were conducted before and after haloperidol (active or placebo) and after placebo and active Δ-9-THC administration (Table 1). Positive, negative, and general symptoms associated with psychosis were assessed using relevant subscales of the Positive and Negative Syndrome Scale (PANSS; Kay et al. 1989), perceptual alterations were measured using the Clinician-administered Dissociative Symptoms Scale (CADSS; Bremner et al. 1998), and feeling states associated with cannabis intoxication were measured using a self-reported visual analog scale of five items (“high,” “calm and relaxed,” “tired,” “panic,” and “anxious”; Haertzen 1965, 1966). Subjects were also asked to rate on a 0–100 scale (0 = not at all to 100 = most of all) (1) the similarity of the experience compared to recreational cannabis use and (2) how much they enjoyed the experience. Inter-rater reliability sessions were conducted every 1–2 months, and, for example, intraclass correlation coefficient for the PANSS were consistently greater than 0.85.
A cognitive test battery was administered 30 min after receiving both placebo and active Δ-9-THC infusions. Learning and recall were measured using the Hopkins Verbal Learning Test (Brandt et al. 1992; Bylsma et al. 1991). This test consists of three consecutive trials of immediate free recall of a 12-item, semantically categorized list, followed 30 min later by testing of delayed free, cued, and recognition recall. Different but equivalent versions of the test were administered within and across test days. Vigilance and distractibility to visual stimuli were measured using a continuous performance task (Gordon 1986) in which subjects attended to numbers presented sequentially on a screen. The subject pushed a button to signal when a ‘1’ was followed by a ‘9.’ The distractibility task was identical to the vigilance task with the exception that numbers were presented sequentially in three contiguous columns. Subjects were instructed to attend to the middle column and ignore the outer two columns.
Executive function (Stockings of Cambridge: SOC), spatial working memory (SWM), visual recognition memory (delayed match to sample: DMTS), and motor screening were tested using the Cambridge Neuroscience Test Battery (CANTAB; http://www.camcog.com; Sahakian and Owen 1992). Intelligence quotient was remeasured as part of the CANTAB using the National Adult Reading Test (NART). A motor-screening task (MOT) was administered to ensure that subjects could point accurately and also to measure speed and accuracy, both of which are indices of motor skill. A series of crosses were shown in different locations on the screen. After a demonstration, the subject had to point to the crosses in turn. The time taken for the subject to touch the cross after it appeared was measured as MOT latency. The arithmetic mean was calculated from the latencies of the ten crosses presented, which were correctly responded to. The DMTS tests visual memory in a four-choice delayed recognition memory paradigm. Subjects were shown a complex visual pattern (the sample). After a variable delay (of 0, 4, or 12 s), three distractor patterns and the target pattern were shown (Robbins et al. 1994). Subjects were instructed to choose the target pattern. The number of occasions upon which the subject selected the correct targets in trials was calculated as a percentage (DMTS percent correct score). In the SWM task, subjects had to find individually hidden “blue tokens” without returning to a box where one had previously been found (Owen et al. 1990). Errors included selecting boxes that had previously been found to be empty (within errors) and revisiting boxes that had already been found to contain a token (between errors). The SOC test is a spatial-planning task based upon the “Tower of London” test. Subjects had to move a set of balls to replicate a reference pattern. The number of occasions that a subject successfully replicated a reference pattern in the minimum possible number of moves was measured. CANTAB tests have satisfactory levels of test–retest reliability, with some outcome measures reaching correlations of better than 0.9. All the CANTAB tests used had parallel versions to facilitate repeated testing, and further, the tests tapped nonstrategic cognitive functions, which are less likely to be subject to significant practice effects.
Akathisia and drug-induced Parkinsonism were evaluated using the Barnes akathisia scale (Barnes 1989) and the Simpson Angus Scale (Simpson and Angus 1970), respectively. However, as subjects were not allowed to ambulate during testing because of safety concerns, the latter was modified to include only the items for tremor and a composite rigidity score (shoulders, elbows, wrist, head rotation) as described elsewhere (D’Souza et al. 2005).
Vital signs were recorded periodically, and blood was sampled for prolactin and cortisol from the intravenous line opposite to the one used for administering the study drug, to provide a behaviorally independent measure of cannabinoid effects. Immediately after collection, blood samples were placed on ice and centrifuged, and the extracted plasma was aliquoted into vials for storage at −70°C until the time of the assay. Prolactin and cortisol assays were run in duplicate pairs using radioimmunoassay kits to determine prolactin (Serono Diagnostics) and cortisol (Baxter Travenol Diagnostics) levels.
Statistical analyses
Initially, data were examined descriptively using means, standard deviations, and graphs. Each outcome was tested for normality using Kolmogorov–Smirnov test statistics and normal probability plots. Some, but not other, outcomes were approximately normal. Some of the skewed data were successfully normalized by log transformation. However, some skewed data could not be normalized by log transformation. These non-normal outcomes were analyzed using the nonparametric approach for repeated measures data (Brunner et al. 2002), where the data were first ranked and then fitted using a mixed-effects model with an unstructured variance–covariance matrix and p values adjusted for analysis of variance-type statistics (ATS). Linear mixed models were used to analyze normal or normalized (log-transformed) data. If data required normalization or could not be normalized, it is specified in “Results.” For all the CANTAB data, vigilance and distractibility data, and the verbal recall models, each outcome, in turn, represented the dependent variable, while haloperidol (placebo vs active) and THC (placebo vs active) were included as within-subject explanatory factors, and group (frequent users vs healthy subjects) was included as a between-subjects factor. However, because no group differences were found, group was eliminated from the models for most of the outcomes except for endocrine, immediate recall, and SWM data. In addition, all CANTAB models were controlled for NART-IQ and motor function (latency). For verbal immediate recall, trial (1–3) was included as an additional within-subject factor. These models allowed for testing of all main and interaction effects of haloperidol and THC. When appropriate, post-hoc comparisons were performed. In the above models, subject was used as the clustering factor. Similar models as above were used to evaluate CADSS, PANSS, and VAS outcomes, except that the THC factor was replaced by time (−90, −30, 15, 65, 140, 190) as a within-subject factor. Data on the similarity to cannabis and enjoyment of the experience were analyzed similarly except that measurements were taken only at time 65 and 190. Because there was little or no variance at earlier time points, analyses of the akathisia and Parkinsonism data were restricted to time 140 only; these models included only the within-subject factor haloperidol. Data were analyzed using SAS, version 9.1 (SAS Institute, Cary, NC). All results were considered statistically significant at P < 0.05. Bonferroni correction was applied within but not across hypotheses. Thus, for the positive symptoms subscale of the PANSS, a cutoff alpha level of 0.05/2 = 0.025 was used to declare effects significant for PANSS positive.
Results
Of the 54 subjects who were screened, a total of 28 subjects (17 healthy subjects and 11 frequent users of cannabis) initiated the study (Table 2). Frequent users and healthy subjects were not significantly different across several measures except for years of education (Table 2) and cannabis use histories (Table 3). However, because there were no group differences found across most outcome measures, unless otherwise specified, the results are presented below for the combined sample. Eight subjects (five healthy subjects and three frequent users) did not complete the study because they disliked the psychotomimetic and anxiogenic effects of Δ-9-THC (n = 2), scheduling difficulties (n = 1), and/or nonstudy issues (n = 5). One subject who did not disclose a history of migraine at screening experienced a headache on the placebo condition. No serious adverse events occurred during the study or during the follow-up period, as determined by face-to-face contact and telephone interview.
Psychotomimetic effects
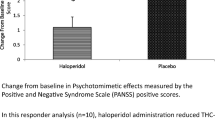
PANSS and CADSS data were highly skewed. Δ-9-THC produced significant increases in PANSS Total (ATS = 24.7, num df = 2.9, unadjusted P < 0.0001), PANSS positive symptoms subscale (ATS = 10.1, num df = 2.8, adjusted P < 0.0001), CADSS subjective [ATS = 15.9, num df = 3.5, unadjusted P < 0.0001), and CADSS objective (ATS = 20.8, num df = 2.9, P < 0.0001) scores. There were no significant effects of haloperidol or haloperidol by Δ-9-THC-interactive effects on any of these outcomes (Fig. 1a and b).

a Positive symptoms of psychosis measured by the Positive Symptoms subscale of the Positive and Negative Syndrome Scale (PANSS). b Perceptual Alterations measured by the Subject rated subscale of the Clinician Administered Dissociative Symptoms Scale (CADSS). c “High” measured by the visual analog scale (VAS). d “Tired” measured by the visual analog scale (VAS; T bars indicate SEMs)
Visual analog scale feeling states
VAS “high,” “anxious,” and “panic” data were highly skewed, while “calm and relaxed” and “tired” data were approximately normal. Δ-9-THC produced significant increases in VAS “high” (ATS = 44.6, num df = 3.2, P < 0.0001) and “tired” (F[5, 27] = 5.01, P = 0.0022) but did not significantly change any other feeling states. There were no significant effects of haloperidol or haloperidol by Δ-9-THC-interactive effects on any of these outcomes (Fig. 1c and d).
Similarity to cannabis and enjoyment of the experience
Data on these measures were skewed (Table 4). Δ-9-THC produced significant increases in ratings of the similarity of the experience to cannabis (ATS = 116.5, num df = 1, P < 0.0001) and enjoyment of the experience (ATS = 41.7, num df = 1, P < 0.0001). Haloperidol reduced ratings of enjoyment of the experience (ATS = 8.0, num df = 1, P = 0.005). There were no significant interactive effects of haloperidol and Δ-9-THC.
Verbal learning and recall
Immediate recall data were approximately normal while all other outcomes were highly skewed.
No significant practice effects both within and across test days were detected on verbal recall or any of the other cognitive measures (Table 4).
Immediate recall
Δ-9-THC significantly impaired immediate total recall (F[1, 27] = 12.49, P = 0.0015). Recall improved significantly across trials (learning) (F[2, 54] = 145.9, P = 0.0001). There was a trend toward a significant interaction between haloperidol and Δ-9-THC (F[1, 19] = 3.4, P = 0.08) with the haloperidol further worsening Δ-9-THC-induced recall deficits. There was a significant three-way interaction between haloperidol, Δ-9-THC, and group (F[1, 18] = 6.0, P = 0.025); this was a result of the combined effect of haloperidol and Δ-9-THC in producing significant recall deficits in healthy subjects (F[1, 18] = 10.43, P = 0.0046) but not in frequent users (F[1, 18] = 2.66, P = 0.12; Fig. 2).

Immediate verbal recall measured by the Hopkins Verbal Learning Task (T bars indicate SEMs). Δ-9-THC impaired immediate recall and haloperidol worsened Δ-9-THC induced immediate recall impairments
Delayed free, cued, and recognition recall
Δ-9-THC (ATS = 8.9, num df = 1, P = 0.0028) and haloperidol (ATS = 3.6, num df = 1, P = 0.056) impaired delayed free recall. Δ-9-THC but not haloperidol impaired delayed cued recall (ATS = 5.6, num df = 1, P = 0.0185). The interaction between haloperidol and Δ-9-THC was significant for delayed free recall (ATS = 4.2, num df = 1, P = 0.04) and delayed cued recall (ATS = 8.9, num df = 1, P = 0.003) with both effects explained by haloperidol further worsening Δ-9-THC-induced recall impairments. Neither Δ-9-THC nor haloperidol impaired delayed recognition recall (Fig. 3).

Delayed verbal recall measured by the Hopkins Verbal Learning Task (T bars indicate SEMs). Δ-9-THC impaired delayed free recall and haloperidol worsened Δ-9-THC induced delayed free recall impairments
Errors
Δ-9-THC significantly increased the number of intrusions (ATS = 7.9, num df = 1, P = 0.005) and false-positive (ATS = 22.1, num df = 1, P < 0.0001) responses but not perseverations. The interaction between haloperidol and Δ-9-THC trended to increase false-positive responses (ATS = 3.5, num df = 1, P = 0.06) with the effects explained by haloperidol further increasing Δ-9-THC false-positive responses.
Attention
Both vigilance and distractibility data were highly skewed (Table 4).
Vigilance
Haloperidol (ATS = 4.4, num df = 1, P = 0.037) and the interaction of Δ-9-THC and haloperidol (ATS = 5.4, num df = 1, P = 0.02) but not Δ-9-THC alone significantly increased omission errors. There were no significant effects of Δ-9-THC, haloperidol, or group on commission errors (Fig. 4a and b).

a, b Vigilance omission and commission errors measured by the Gordon Box Continuous Performance Task (CPT). Haldol alone and in combination with Δ-9-THC increased omission errors. c, d Distractibility omission and commission errors measured by the Gordon Box CPT. Δ-9-THC alone and haloperidol alone increased omission and commission errors. T bars indicate SEMs
Distractibility
Δ-9-THC (ATS = 10.0, num df = 1, P = 0.0016), haloperidol (ATS = 25.6, num df = 1, P < 0.0001), and the interaction of Δ-9-THC and haloperidol (ATS = 7.0, num df = 1, P = 0.008) significantly increased omission errors. The latter was driven by the effects of haloperidol. Haloperidol significantly (ATS = 6.1, num df = 1, P = 0.014) and Δ-9-THC trended (ATS = 3.5, num df = 1, P = 0.06) to increase commission errors, but there were no significant interactive effects between the two (Fig. 4c and d).
CANTAB
Motor screening
Δ-9-THC (F[1, 64] = 6.4, P = 0.01) but not haloperidol or the interactions between the two significantly reduced mean latency motor performance (Table 4).
Spatial working memory
Between-errors data were normalized by log transformation. Δ-9-THC increased between (F[1, 26] = 5.2, P = 0.03) but not within errors, while haloperidol had no effects on either type of error. This was one of the few measures where there was a significant interactive effect of group and Δ-9-THC on between errors (F[1, 25] = 4.2, P = 0.05); this was due to healthy subjects having higher Δ-9-THC induced between errors (F[1, 25] = 9.88, P = 0.004; Fig. 5).

Spatial working memory measured by the CANTAB (Cambridge Neuroscience Battery; T bars indicate SEMs). Δ-9-THC and the combination of Δ-9-THC increased between errors only in healthy subjects
Stockings of Cambridge
There were no significant effects of Δ-9-THC, haloperidol, group, or any interactions between the two on the number of occasions that subjects successfully replicated a reference pattern in the minimum possible number of moves.
Delayed match to sample task
Haloperidol significantly reduced percent correct performance (F[1, 62] = 6.0, P = 0.017). There were no effects of Δ-9-THC, group, or any interactions between Δ-9-THC, group, or haloperidol on any of the measures.
Akathisia, rigidity, and tremor
All outcomes were highly skewed. Δ-9-THC (ATS = 5.1, num df = 1.6, P < 0.0098) but not haloperidol increased Barnes Global Akathisia scores. Neither Δ-9-THC nor haloperidol had any effect on tremor or rigidity (see Table S1 in Electronic supplementary material). There were no significant effects of haloperidol or group or the interactions between haloperidol, Δ-9-THC, and group on any of the other motor outcomes.
Neuroendocrine effects
Prolactin and cortisol levels were approximately normally distributed after log transformation. Serum cortisol levels decreased over time (F[2, 107] = 51.05, P < 0.0001), but there were no significant effects of haloperidol or interactions between haloperidol and Δ-9-THC (Fig. 6).

Plasma prolactin levels (T bars indicate SEMs). Lower baseline prolactin levels in frequent users. Haloperidol but not Δ-9-THC increases prolactin levels
Haloperidol increased (F[1, 107] = 77.7, P < 0.0001) and time/Δ-9-THC decreased (F[2, 107] = 10.8, P ≤ 0.0001) serum prolactin levels. The interaction between haloperidol and time/Δ-9-THC was significant (F[2, 107] = 56.8, P < 0.0001) where prolactin levels on the active haloperidol condition were significantly greater at 65 (F[1, 107] = 15.8, P = 0.0001) and 190 min (F[1, 107] = 144.5, P < 0.0001) but not at baseline (not significant). Of note, serum prolactin levels were lower in frequent users of cannabis (F[1, 102] = 7.1, P = 0.009).
Discussion
This is the first published report to our knowledge on the interactions between haloperidol and Δ-9-THC in humans. The principal finding of this study is that haloperidol, at a dose that produced effects consistent, e.g., with prolactin elevation with acute antagonism of DA D2 receptors, failed to reduce any Δ-9-THC effects. Instead, haloperidol worsened some of the cognitive effects of Δ-9-THC.
Effects of haloperidol alone
Haloperidol worsened performance on some cognitive tasks similar to other reports (Saeedi et al. 2006). As expected, haloperidol increased serum prolactin levels. In addition, the observation that haloperidol did not produce any obvious behavioral or motor effects confirms the appropriateness of the dose that was selected. At this dose, most of haloperidol’s effects would be expected to be related to its antagonism of DA D2 receptors. Its affinity for histaminic H1 and muscarinic M1 receptors is greater than 600 and greater than 2,000 times less than its affinity for DA D2 receptors. Similarly, any interactions between Δ-9-THC and haloperidol most likely converge through DAergic systems.
Effects of Δ-9-THC alone
The dose and rate of Δ-9-THC administration in this study were chosen in an attempt to mimic recreational cannabis use. The observation that subjects reported that the experience was similar to cannabis and that they enjoyed it supports the generalizability of the findings to recreational cannabis use.
The effects of intravenous Δ-9-THC observed in this study were similar to but of smaller magnitude than the effects produced by higher doses of intravenous Δ-9-THC (2.5 and 5 mg over 2 min; D’Souza et al. 2004, 2005, 2006). For example, the Δ-9-THC dose (2 mg over 20 min in a 70-kg individual) in this study produced peak self-rated perceptual alteration CADSS score (3.96) nearly four times lower than the effects (14.95) of a higher Δ-9-THC dose (5 mg over 2 min) (D’Souza et al. 2004). Nevertheless, the peak increases in PANSS positive symptoms scores induced by this Δ-9-THC dosing paradigm were comparable to the peak increases in positive symptom scores induced by (1) amphetamine 0.25 mg/kg administered i.v. over 1 min (Krystal et al. 2005), (2) low-dose ketamine (bolus 0.081 mg/kg over 10 min followed by an infusion of 0.4 mg kg−1 h−1; Krystal et al. 2006), and m-chlorphenylpiperazine (D’Souza et al. 2006). As discussed earlier, we attempted a shorter infusion and higher dose of Δ-9-THC in combination with haloperidol, but this was poorly tolerated.
Some of the cognitive effects of Δ-9-THC that have been well described in animals but not in humans were measured in this study. Cannabinoids impair spatial memory in animals (Aigner 1988; Carlini et al. 1970a, b; Winsauer et al. 1999), and we now show for the first time in humans that Δ-9-THC impairs SWM as evidenced by an increase in between but not within errors. This profile of effects suggests that while subjects were able to perform the basic task, the longer they had to maintain information online, the worse they performed. Further, the observation that Δ-9-THC did not impair performance in frequent users of cannabis (Fig. 5) is consistent with the preclinical observations of tolerance to the effects of cannabinoids on SWM (Lichtman et al. 1995). Further, the absence of an effect in frequent users of cannabis is important to consider in interpreting the cannabis literature, as most studies have included frequent or heavy users of cannabis. Finally, the observation of group differences only on the SWM task suggests that the latter may be most sensitive in detecting differences between frequent users and healthy subjects.
In animals, cannabinoids impair performance on the DMTS, a visual recognition memory task, only when the delay is long (Heyser et al. 1993; Winsauer et al. 1999). Δ-9-THC did not impair DMTS in this study even when the delay was long. Other studies of Δ-9-THC on DMTS performance have had mixed results (Heishman et al. 1997; Lane et al. 2005). Perhaps, differences in the delay periods, other task parameters, Δ-9-THC doses, and degree of cannabinoid tolerance across samples might account for the disparate results. Consistent with a wealth of clinical data (reviewed in Ranganathan and D’Souza 2006), Δ-9-THC impaired several aspects of verbal recall. The fact that Δ-9-THC impaired free verbal recall but not visual and verbal recognition recall suggests that Δ-9-THC does not impair encoding but rather impairs retrieval and/or consolidation.
While Δ-9-THC reduced the number of problems solved in minimum moves on the SOC task (Table 5), these effects were not statistically significant. Of note, Ramaekers et al. (2006) showed that higher doses of Δ-9-THC impair performance on a task analogous to the SOC, the Tower of London task. They went on to argue that Δ-9-THC effects on executive function may be relatively small at low doses, similar to those used in this study, but may become “very substantial” at higher doses.
Δ-9-THC also reduced motor latency. Others have reported that Δ-9-THC produces an increase in the speed of responding along with worse performance suggesting that under the influence of cannabinoids, individuals trade speed for accuracy (Curran et al. 2002).
Interactive effects of haloperidol and Δ-9-THC
Behavioral and subjective outcomes
While both PANSS positive symptoms (Fig. 1a) and CADSS perceptual alterations (Fig. 1b) scores induced by Δ-9-THC were lower on the active vs the placebo haloperidol condition (see Table 4), these effects were not statistically significant. These results are not consistent with the report that “cannabis-induced psychosis” is responsive to treatment with DA D2 receptor antagonists (Berk et al. 1999). In contrast, the current results are consistent with the observation that Δ-9-THC increased psychotomimetic symptoms in schizophrenic patients despite chronic treatment with DA D2 receptor antagonists (D’Souza et al. 2005). Perhaps, the effects of Δ-9-THC better model those positive symptoms that are resistant to DA D2 receptor antagonist antipsychotic drugs. Further, whereas Δ-9-THC produces positive and negative symptoms and cognitive deficits (D’Souza et al. 2004, 2005), amphetamine produces predominantly positive symptoms (Angrist et al. 1974b; Angrist and Gershon 1970; Griffith et al. 1972). Finally, haloperidol reverses psychosis induced by amphetamine (Angrist et al. 1974a). However, haloperidol pretreatment did not reduce the psychosis induced by ketamine (Krystal et al. 1999), lysergic acid diethylamide, and, in the current study, Δ-9-THC. Taken collectively, this suggests that DA D2 mechanisms may not play a major role in the pathophysiology of Δ-9-THC-induced psychotomimetic effects. Perhaps, the use of a single and relatively low dose of haloperidol combined with the small increases in Δ-9-THC-induced psychotomimetic symptoms may explain the lack of a haloperidol effect in this study. Alternatively, the failure of haloperidol to block Δ-9-THC-induced psychotomimetic effects reflects a limitation in the relevance of the cannabinoid “model” of psychosis.
Similarly, the lack of any effect of haloperidol on Δ-9-THC-induced VAS measured subjective effects (“high,” “tired,” etc.) is consistent with our observations that chronic antipsychotic treatment did not blunt the euphoric effects of Δ-9-THC in schizophrenic patients (D’Souza et al. 2005). The failure of haloperidol to block the euphoric effects of Δ-9-THC was surprising given that the rewarding properties of cannabinoids, like other drugs of abuse, have been associated with an increased activity of mesolimbic DA transmission (Chen et al. 1990b, 1991; Fadda et al. 2006; French 1997; French et al. 1997; Ng Cheong Ton et al. 1988; Patel and Hillard 2003; Tanda et al. 1997a, b). Relevant to both the euphoric and psychotomimetic effects of Δ-9-THC, the DA D2 receptor antagonist sulpiride failed to block Δ-9-THC-induced c-fos expression in both the striatum and nucleus accumbens (Miyamoto et al. 1996). Regardless, the current findings suggest that acute DA D2 receptor blockade antagonists may not be useful in cannabis addiction or psychosis, but whether repeated dosing is useful remains unclear.
Cognitive outcomes
Together, haloperidol and Δ-9-THC impaired sustained attention (increased omission errors on both vigilance and distractibility tasks) and immediate and delayed verbal recall. Further, while the interactive effects of haloperidol and Δ-9-THC on visual recognition memory, SWM, and planning and execution did not reach statistical significance, the effects were in the direction of the combination of the two drugs worsening performance to a greater extent than either drug alone. The observed findings were not predicted and at present can only be speculated upon. Attention, execution function, visual recognition memory, SWM, verbal learning, and recall all require varying contributions of and complex interactions between the prefrontal cortex (PFC) and hippocampus. For instance, cannabinoids could alter PFC and hippocampal function via their effects on the release of DA, acetylcholine, glutamate, or norepinephrine. While it is out of the scope of this paper to discuss all these possibilities, we briefly discuss some of the preclinical evidence of crosstalk between CB1 and DA systems in the PFC, which might explain some of the interactive cognitive effects of haloperidol and Δ-9-THC.
Systemically administered cannabinoids can modulate the activity of DAergic pathways in the PFC either directly or indirectly, by influencing the activity of DAergic neurons through either post- or presynaptic mechanisms (Egerton et al. 2006; Laviolette and Grace 2006b; Pistis et al. 2002). CB-induced DAergic hyperactivity in the PFC may contribute to working memory deficits associated with CB exposure (Diana et al. 1998; Jentsch et al. 1997). Acute administration of haloperidol may result in acute DA D2 blockade but also compensatory DA release in the medial PFC and nucleus accumbens (Liegeois et al. 2002; Moghaddam and Bunney 1990; Moghaddam et al. 1990). Thus, the combination of Δ-9-THC and haloperidol may result in additive DA release in the PFC. Given that either too high or low DAergic activity in the PFC can lead to impairments in PFC-related cognitive functions (Goldman-Rakic 1996; Murphy et al. 1996; Zahrt et al. 1997), this may explain the observations that the combination of haloperidol and Δ-9-THC worsened cognition.
Prolactin
Δ-9-THC produces an early and brief increase followed by a predominantly inhibitory effect on prolactin release (Harclerode 1984; Murphy et al. 1998) that is believed to be mediated by CB-1R activation of tuberoinfundibular (TIDA) DA neurons (Rodriguez De Fonseca et al. 1992). Of note, frequent users of cannabis had lower prolactin levels. Prolactin release is under tonic DA control (Selmanoff 1981), and prolactin controls its own release by altering DA release (Gregerson and Selmanoff 1988). Thus, the lower-baseline prolactin levels in frequent users may reflect increased DA tone in the TIDA pathway of frequent users that is related to either residual cannabis effects or long-term adaptive changes in DA function in response to chronic cannabis exposure. In a previous study, 5 mg but not 2.5 mg Δ-9-THC increased prolactin levels in healthy human subjects (D’Souza et al. 2004). Perhaps, the lack of a significant acute effect of Δ-9-THC on plasma prolactin in this study may be explained by the small dose (2 mg) and limited sampling.
Limitations
There were several limitations to this study. First, the use of multiple doses of haloperidol and Δ-9-THC may have been more informative than the current design but was not feasible, as discussed earlier. Second, because haloperidol has affinity for other receptors (D1 and α1), any interactions of Δ-9-THC and haloperidol cannot be attributed solely to interactions with D2 receptors. Third, the smaller magnitude of Δ-9-THC induced behavioral and cognitive effects in this study compared to previous studies, which used higher doses and a faster infusion (D’Souza et al. 2004, 2005), may have reduced the likelihood of detecting a beneficial effect of haloperidol. Fourth, the limited sample size may, in part, contribute to the lack of significant findings. For example, the difference in Δ-9-THC-induced increase in PANSS positive symptom score between the placebo and active haloperidol test days was 0.65 (SD 1.56). This translates into a small to medium effect size (d = 0.42) for the reduction in Δ-9-THC-induced positive symptoms, which, with 28 subjects, would not be adequately powered to detect. However, with 28 subjects, we still had 80% statistical power to detect medium/large effects size (d = 0.55) with 80% statistical power for any given outcome. Fifth, a random order of Δ-9-THC (placebo or active) administration would have been preferred. Sixth, in contrast to the cognitive assessments, the behavioral and subjective effects were measured repeatedly during each Δ-9-THC session. This should be noted in interpreting the effects of haloperidol pretreatment on Δ-9-THC effects.
Conclusions
The current study replicates a growing body of research characterizing the cognitive effects, perceptual altering, psychotomimetic, and euphoric of Δ-9-THC. The failure of haloperidol pretreatment to antagonize the psychotomimetic effects of Δ-9-THC suggests that these effects of Δ-9-THC are not likely mediated by DA D2 receptor mechanisms and that novel pharmacologic approaches will be needed to block these effects. Given the growing interest in the link between cannabinoids and psychosis, future research should be directed toward understanding the precise mechanisms underlying the psychotomimetic symptoms produced by Δ-9-THC. While admittedly speculative, the search for drugs that block the psychotomimetic symptoms produced by Δ-9-THC may lead to novel approaches to the treatment of psychotic disorders. The deleterious effect of haloperidol pretreatment on the cognitive effects of Δ-9-THC is consistent with the preclinical literature in suggesting crosstalk between DAergic and CBergic systems. However, further work is necessary to fully understand the crosstalk between the two systems in humans.
References
Agurell S, Halldin M, Lindgren JE, Ohlsson A, Widman M, Gillespie H, Hollister L (1986) Pharmacokinetics and metabolism of delta 1-tetrahydrocannabinol and other cannabinoids with emphasis on man. Pharmacol Rev 38:21–43
Aigner TG (1988) Delta-9-tetrahydrocannabinol impairs visual recognition memory but not discrimination learning in rhesus monkeys. Psychopharmacology 95:507–511
Angrist BM, Gershon S (1970) The phenomenology of experimentally induced amphetamine psychosis–preliminary observations. Biol Psychiatry 2:95–107
Angrist B, Lee HK, Gershon S (1974a) The antagonism of amphetamine-induced symptomatology by a neuroleptic. Am J Psychiatry 131:817–819
Angrist B, Sathananthan G, Wilk S, Gershon S (1974b) Amphetamine psychosis: behavioral and biochemical aspects. J Psychiatr Res 11:13–23
Barnes TR (1989) A rating scale for drug-induced akathisia. Br J Psychiatry 154:672–676
Berk M, Brook S, Trandafir AI (1999) A comparison of olanzapine with haloperidol in cannabis-induced psychotic disorder: a double-blind randomized controlled trial. Int Clin Psychopharmacol 14:177–1780
Brandt J, Corwin J, Krafft L (1992) Is verbal recognition memory really different in Huntington’s and Alzheimer’s disease. J Clin Exp Neuropsychol 14:773–784
Bremner JD, Krystal JH, Putnam FW, Southwick SM, Marmar C, Charney DS, Mazure CM (1998) Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J Trauma Stress 11:125–136
Brunner E, Domhof S, Langer F (2002) Nonparametric analysis of longitudinal data in factorial experiments. Wiley, New York
Budney AJ, Moore BA, Vandrey RG, Hughes JR (2003) The time course and significance of cannabis withdrawal. J Abnorm Psychology 112:393–402
Bylsma FW, Rebok GW, Brandt J (1991) Long-term retention of implicit learning in Huntington’s disease. Neuropsychologia 29:1213–1221
Carlini EA, Hamaoui A, Bieniek D, Korte F (1970a) Effects of (−) delta-9-trans-tetrahydrocannabinol and a synthetic derivative on maze performance of rats. Pharmacology 4:359–368
Carlini EA, Santos M, Claussen U, Bieniek D, Korte F (1970b) Structure activity relationship of four tetrahydrocannabinols and the pharmacological activity of five semi-purified extracts of Cannabis sativa. Psychopharmacologia 18:82–93
Chen J, Paredes W, Lowinson JH, Gardner EL (1990a) Delta 9-tetrahydrocannabinol enhances presynaptic dopamine efflux in medial prefrontal cortex. Eur J Pharmacol 190:259–262
Chen JP, Paredes W, Li J, Smith D, Lowinson J, Gardner EL (1990b) Delta 9-tetrahydrocannabinol produces naloxone-blockable enhancement of presynaptic basal dopamine efflux in nucleus accumbens of conscious, freely-moving rats as measured by intracerebral microdialysis. Psychopharmacology 102:156–162
Chen JP, Paredes W, Lowinson JH, Gardner EL (1991) Strain-specific facilitation of dopamine efflux by delta 9-tetrahydrocannabinol in the nucleus accumbens of rat: an in vivo microdialysis study. Neurosci Lett 129:136–180
Compton WM, Grant BF, Colliver JD, Glantz MD, Stinson FS (2004) Prevalence of marijuana use disorders in the United States: 1991–1992 and 2001–2002. Jama 291:2114–2121
Curran HV, Brignell C, Fletcher S, Middleton P, Henry J (2002) Cognitive and subjective dose-response effects of acute oral Delta 9-tetrahydrocannabinol (THC) in infrequent cannabis users. Psychopharmacology 164:61–70
D’Souza DC (2007) Cannabinoids and psychosis. Int Rev Neurobiol 78:289–326
D’Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Wu YT, Braley G, Gueorguieva R, Krystal JH (2004) The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology 29:1558–1572
D’Souza DC, Abi-Saab WM, Madonick S, Forselius-Bielen K, Doersch A, Braley G, Gueorguieva R, Cooper TB, Krystal JH (2005) Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry 57:594–608
D’Souza DC, Gil RB, Zuzarte E, MacDougall LM, Donahue L, Ebersole JS, Boutros NN, Cooper T, Seibyl J, Krystal JH (2006) Gamma-aminobutyric acid-serotonin interactions in healthy men: implications for network models of psychosis and dissociation. Biol Psychiatry 59:128–137
D’Souza DC, Ranganathan M, Braley G, Gueorguieva R, Zimolo Z, Cooper T, Perry E, Krystal J (2008) Blunted Psychotomimetic and Amnestic Effects of Delta-9-tetrahydrocannabinol in Frequent Users of Cannabis. Neuropsychopharmacology (in press). DOI 10.1038/sj.npp.1301643
Diana M, Melis M, Gessa GL (1998) Increase in meso-prefrontal dopaminergic activity after stimulation of CB1 receptors by cannabinoids. Eur J Neurosci 10:2825–2830
Egerton A, Allison C, Brett RR, Pratt JA (2006) Cannabinoids and prefrontal cortical function: insights from preclinical studies. Neurosci Biobehav Rev 30:680–695
Fadda P, Scherma M, Spano MS, Salis P, Melis V, Fattore L, Fratta W (2006) Cannabinoid self-administration increases dopamine release in the nucleus accumbens. Neuroreport 17:1629–1632
Farde L, Nordstrom AL, Wiesel FA, Pauli S, Halldin C, Sedvall G (1992) Positron emission tomographic analysis of central D1 and D2 dopamine receptor occupancy in patients treated with classical neuroleptics and clozapine. Relation to extrapyramidal side effects. Arch Gen Psychiatry 49:538–544
Fergusson DM, Poulton R, Smith PF, Boden JM (2006) Cannabis and psychosis. Bmj 332:172–175
First MB, Spitzer RL, Gibbon M, Williams JBW (2002) Structured clinical interview for DSM-IV-TR Axis I disorders—non-patient edition. American Psychiatric Association, Washington, DC
French ED (1997) delta9-Tetrahydrocannabinol excites rat VTA dopamine neurons through activation of cannabinoid CB1 but not opioid receptors. Neurosci Lett 226:159–162
French ED, Dillon K, Wu X (1997) Cannabinoids excite dopamine neurons in the ventral tegmentum and substantia nigra. Neuroreport 8:649–652
Gardner EL (2005) Endocannabinoid signaling system and brain reward: emphasis on dopamine. Pharmacol Biochem Behav 81:263–284
Gessa GL, Melis M, Muntoni AL, Diana M (1998) Cannabinoids activate mesolimbic dopamine neurons by an action on cannabinoid CB1 receptors. Eur J Pharmacol 341:39–44
Goldman-Rakic PS (1996) Regional and cellular fractionation of working memory. Proc Natl Acad Sci USA 93:13473–13480
Gordon M (1986) Microprocessor-based assessment of attention deficit disorders (ADD). Psychopharmacol Bull 22:288–290
Gregerson KA, Selmanoff M (1988) Selective effects of hyperprolactinemia on in vitro dopamine release from median eminence synaptosomes. J Neurosci 8:2477–2484
Griffith JD, Cavanaugh J, Held J, Oates JA (1972) Dextroamphetamine. Evaluation of psychomimetic properties in man. Arch Gen Psychiatry 26:97–100
Haertzen CA (1965) Addiction Research Center Inventory (ARCI): development of a general drug estimation scale. J Nerv Ment Dis 141:300–307
Haertzen CA (1966) Development of scales based on patterns of drug effects, using the addiction Research Center Inventory (ARCI). Psychol Rep 18:163–194
Haney M (2005) The marijuana withdrawal syndrome: diagnosis and treatment. Curr Psychiatry Rep 7:360–366
Haney M, Ward AS, Comer SD, Foltin RW, Fischman MW (1999a) Abstinence symptoms following oral THC administration to humans. Psychopharmacology 141:385–394
Haney M, Ward AS, Comer SD, Foltin RW, Fischman MW (1999b) Abstinence symptoms following smoked marijuana in humans. Psychopharmacology (Berl) 141:395–404
Harclerode J (1984) Endocrine effects of marijuana in the male: preclinical studies. In: Braude MC, Ludford JP (eds) NIDA Research Monograph Series. National Institute on Drug Abuse, Rockville, MD, pp 45–114
Heishman SJ, Arasteh K, Stitzer ML (1997) Comparative effects of alcohol and marijuana on mood, memory, and performance. Pharmacol Biochem Behav 58:93–101
Henquet C, Murray R, Linszen D, van Os J (2005) The environment and schizophrenia: the role of Cannabis use. Schizophr Bull 31:608–612
Henquet C, Rosa A, Krabbendam L, Papiol S, Fananas L, Drukker M, Ramaekers JG, van Os J (2006) An experimental study of catechol-o-methyltransferase Val158Met moderation of delta-9-tetrahydrocannabinol-induced effects on psychosis and cognition. Neuropsychopharmacology 31:2748–2757
Hermann H, Marsicano G, Lutz B (2002) Coexpression of the cannabinoid receptor type 1 with dopamine and serotonin receptors in distinct neuronal subpopulations of the adult mouse forebrain. Neuroscience 109:451–460
Heyser CJ, Hampson RE, Deadwyler SA (1993) Effects of delta-9-tetrahydrocannabinol on delayed match to sample performance in rats: alterations in short-term memory associated with changes in task specific firing of hippocampal cells. J Pharmacol Exp Ther 264:294–307
Jarrahian A, Watts VJ, Barker EL (2004) D2 dopamine receptors modulate Galpha-subunit coupling of the CB1 cannabinoid receptor. J Pharmacol Exp Ther 308:880–886
Jentsch JD, Andrusiak E, Tran A, Bowers MB Jr., Roth RH (1997) Delta 9-tetrahydrocannabinol increases prefrontal cortical catecholaminergic utilization and impairs spatial working memory in the rat: blockade of dopaminergic effects with HA966. Neuropsychopharmacology 16:426–432
Jentsch JD, Verrico CD, Le D, Roth RH (1998) Repeated exposure to delta 9-tetrahydrocannabinol reduces prefrontal cortical dopamine metabolism in the rat. Neurosci Lett 246:169–172
Kapur S, Zipursky R, Roy P, Jones C, Remington G, Reed K, Houle S (1997) The relationship between D2 receptor occupancy and plasma levels on low dose oral haloperidol: a PET study. Psychopharmacology (Berl) 131:148–152
Kapur S, Zipursky R, Jones C, Remington G, Houle S (2000) Relationship between dopamine D(2) occupancy, clinical response, and side effects: a double-blind PET study of first-episode schizophrenia. Am J Psychiatry 157:514–520
Kay SR, Opler LA, Lindenmayer JP (1989) The Positive and Negative Syndrome Scale (PANSS): rationale and standardisation. Br J Psychiatr Suppl 7:59–67
King DJ (1997) Guidelines for the use of antipsychotic drug studies in healthy volunteers. The BAP Consensus Group. J Psychopharmacol 11:201–209
Kinoshita H, Hasegawa T, Katsumata Y, Kameyama T, Yamamoto I, Nabeshima T (1994) Effect of dizocilpine (MK-801) on the catalepsy induced by delta 9-tetrahydrocannabinol in mice. J Neural Transm Gen Sect 95:137–143
Kolb B, Gorny G, Limebeer CL, Parker LA (2006) Chronic treatment with Delta-9-tetrahydrocannabinol alters the structure of neurons in the nucleus accumbens shell and medial prefrontal cortex of rats. Synapse 60:429–436
Krystal JH, D’Souza DC, Karper LP, Bennett A, Abi-Dargham A, Abi-Saab D, Cassello K, Bowers MB Jr., Vegso S, Heninger GR, Charney DS (1999) Interactive effects of subanesthetic ketamine and haloperidol in healthy humans. Psychopharmacology (Berl) 145:193–204
Krystal JH, Perry EB Jr., Gueorguieva R, Belger A, Madonick SH, Abi-Dargham A, Cooper TB, Macdougall L, Abi-Saab W, D’Souza DC (2005) Comparative and interactive human psychopharmacologic effects of ketamine and amphetamine: implications for glutamatergic and dopaminergic model psychoses and cognitive function. Arch Gen Psychiatry 62:985–994
Krystal JH, Madonick S, Perry E, Gueorguieva R, Brush L, Wray Y, Belger A, D’Souza DC (2006) Potentiation of low dose ketamine effects by naltrexone: potential implications for the pharmacotherapy of alcoholism. Neuropsychopharmacology 31:1793–1800
Lane SD, Cherek DR, Lieving LM, Tcheremissine OV (2005) Marijuana effects on human forgetting functions. J Exp Anal Behav 83:67–83
Laviolette SR, Grace AA (2006a) Cannabinoids Potentiate Emotional Learning Plasticity in Neurons of the Medial Prefrontal Cortex through Basolateral Amygdala Inputs. J Neurosci 26:6458–6468
Laviolette SR, Grace AA (2006b) The roles of cannabinoid and dopamine receptor systems in neural emotional learning circuits: implications for schizophrenia and addiction. Cell Mol Life Sci 63:1597–1613
Leweke FM, Schneider U, Thies M, Munte TF, Emrich HM (1999) Effects of synthetic delta9-tetrahydrocannabinol on binocular depth inversion of natural and artificial objects in man. Psychopharmacology (Berl) 142:230–235
Lichtman AH, Martin BR (2005) Cannabinoid tolerance and dependence. Handb Exp Pharmacol 168:691–717
Lichtman AH, Dimen KR, Martin BR (1995) Systemic or intrahippocampal cannabinoid administration impairs spatial memory in rats. Psychopharmacology (Berl) 119:282–290
Liegeois JF, Ichikawa J, Meltzer HY (2002) 5-HT(2A) receptor antagonism potentiates haloperidol-induced dopamine release in rat medial prefrontal cortex and inhibits that in the nucleus accumbens in a dose-dependent manner. Brain Res 947:157–165
Marchese G, Casti P, Ruiu S, Saba P, Sanna A, Casu G, Pani L (2003) Haloperidol, but not clozapine, produces dramatic catalepsy in delta9-THC-treated rats: possible clinical implications. Br J Pharmacol 140:520–526
Martin GW, Wilkinson DA, Kapur BM (1988) Validation of self-reported Cannabis use by urine analysis. Addict Behav 13:147–150
Meschler JP, Howlett AC (2001) Signal transduction interactions between CB1 cannabinoid and dopamine receptors in the rat and monkey striatum. Neuropharmacology 40:918–926
Miyamoto A, Yamamoto T, Ohno M, Watanabe S, Tanaka H, Morimoto S, Shoyama Y (1996) Roles of dopamine D1 receptors in delta 9-tetrahydrocannabinol-induced expression of Fos protein in the rat brain. Brain Res 710:234–240
Moghaddam B, Bunney BS (1990) Acute effects of typical and atypical antipsychotic drugs on the release of dopamine from prefrontal cortex, nucleus accumbens, and striatum of the rat: an in vivo microdialysis study. J Neurochem 54:1755–1760
Moghaddam B, Roth RH, Bunney BS (1990) Characterization of dopamine release in the rat medial prefrontal cortex as assessed by in vivo microdialysis: comparison to the striatum. Neuroscience 36:669–676
Murphy BL, Arnsten AF, Goldman-Rakic PS, Roth RH (1996) Increased dopamine turnover in the prefrontal cortex impairs spatial working memory performance in rats and monkeys. Proc Natl Acad Sci USA 93:1325–1329
Murphy LL, Munoz RM, Adrian BA, Villanua MA (1998) Function of cannabinoid receptors in the neuroendocrine regulation of hormone secretion. Neurobiol Dis 5:432–446
Nagai H, Egashira N, Sano K, Ogata A, Mizuki A, Mishima K, Iwasaki K, Shoyama Y, Nishimura R, Fujiwara M (2006) Antipsychotics improve Delta(9)-tetrahydrocannabinol-induced impairment of the prepulse inhibition of the startle reflex in mice. Pharmacol Biochem Behav 84:330–336
Ng Cheong Ton JM, Gerhardt GA, Friedemann M, Etgen AM, Rose GM, Sharpless NS, Gardner EL (1988) The effects of delta 9-tetrahydrocannabinol on potassium-evoked release of dopamine in the rat caudate nucleus: an in vivo electrochemical and in vivo microdialysis study. Brain Res 451:59–68
Owen AM, Downes JJ, Sahakian BJ, Polkey CE, Robbins TW (1990) Planning and spatial working memory following frontal lobe lesions in man. Neuropsychologia 28:1021–1034
Patel S, Hillard CJ (2003) Cannabinoid-induced Fos expression within A10 dopaminergic neurons. Brain Res 963:15–25
Pistis M, Ferraro L, Pira L, Flore G, Tanganelli S, Gessa GL, Devoto P (2002) Delta(9)-tetrahydrocannabinol decreases extracellular GABA and increases extracellular glutamate and dopamine levels in the rat prefrontal cortex: an in vivo microdialysis study. Brain Res 948:155–158
Ramaekers JG, Kauert G, van Ruitenbeek P, Theunissen EL, Schneider E, Moeller MR (2006) High-potency marijuana impairs executive function and inhibitory motor control. Neuropsychopharmacology 31:2296–2303
Ranganathan M, D’Souza D (2006) the acute effects of cannabinoids on memory in humans: a review. Psychopharmacology 188:425–444
Ranganathan M, Perry E, Braley G, Cooper T, Gueorguieva R, Krystal J, D’Souza DC (2007) Blunted “negative” but not “positive” effects of thc in cannabis abusers: implications for cannabis use in schizophrenia. In: Schulz CTaC (ed) International Congress on Schizophrenia Research. Schizophrenia Bulletin, Colorado Springs, p 477
Robbins TW, James M, Owen AM, Sahakian BJ, McInnes L, Rabbitt P (1994) Cambridge Neuropsychological Test Automated Battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dementia 5:266–281
Rodriguez De Fonseca F, Fernandez-Ruiz JJ, Murphy LL, Cebeira M, Steger RW, Bartke A, Ramos JA (1992) Acute effects of delta-9-tetrahydrocannabinol on dopaminergic activity in several rat brain areas. Pharmacol Biochem Behav 42:269–275
Saeedi H, Remington G, Christensen BK (2006) Impact of haloperidol, a dopamine D2 antagonist, on cognition and mood. Schizophr Res 85:222–231
Sahakian BJ, Owen AM (1992) Computerized assessment in neuropsychiatry using CANTAB: discussion paper. J R Soc Med 85:399–402
SAMHSA (2004) Results from the 2003 National Survey on Drug Use and Health: national findings. Substance Abuse and Mental Health Services AdministrationRockville, MD
Schotte A, Janssen PF, Gommeren W, Luyten WH, Van Gompel P, Lesage AS, De Loore K, Leysen JE (1996) Risperidone compared with new and reference antipsychotic drugs: in vitro and in vivo receptor binding. Psychopharmacology (Berl) 124:57–73
Selmanoff M (1981) The lateral and medial median eminence: distribution of dopamine, norepinephrine, and luteinizing hormone-releasing hormone and the effect of prolactin on catecholamine turnover. Endocrinology 108:1716–1722
Simpson GM, Angus JW (1970) A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl 212:11–19
Sobell LC, Sobell MB (1992) Timeline follow-back: a technique for assessing self-reported alcohol consumption. In: Litten R, Allen J (eds) Measuring alcohol consumption. Humana, Totowa, NJ, pp 41–72
Spitzer RL, Williams JBW, Gibbon M, First MB (1990) Structured clinical interview for DSM-III-R-patient edition (SCID-P, version 1.0). American Psychiatric, Washington, DC
Tanda G, Pontieri FE, Di Chiara G (1997a) Cannabinoid and heroin activation of mesolimbic dopamine transmission by a common mu1 opioid receptor mechanism. Science 276:2048–2050
Tanda G, Pontieri FE, Di Chiara G (1997b) Cannabinoid and heroin activation of mesolimbic dopamine transmission by a common mu1 opioid receptor mechanism [comment]. Science 276:2048–2050
Verrico CD, Jentsch JD, Roth RH (2003) Persistent and anatomically selective reduction in prefrontal cortical dopamine metabolism after repeated, intermittent cannabinoid administration to rats. Synapse 49:61–66
Wachtel SR, ElSohly MA, Ross SA, Ambre J, de Wit H (2002) Comparison of the subjective effects of Delta(9)-tetrahydrocannabinol and marijuana in humans. Psychopharmacology (Berl) 161:331–339
Wall ME, Brine DR, Perez-Reyes M (1976) Metabolism of cannabinoids in man. In: Braude MC, Szara S (eds) Pharmacology of marihuana. vol. 1. Raven, New York (536pp.)
Winsauer PJ, Lambert P, Moerschbaecher JM (1999) Cannabinoid ligands and their effects on learning and performance in rhesus monkeys. Behav Pharmacol 10:497–511
Zahrt J, Taylor JR, Mathew RG, Arnsten AF (1997) Supranormal stimulation of D1 dopamine receptors in the rodent prefrontal cortex impairs spatial working memory performance. J Neurosci 17:8528–8535
Acknowledgements
The authors wish to acknowledge the critical clinical research contributions of the Biological Studies Unit, VA Connecticut Healthcare System, including Elizabeth O’Donell, R.N; Angelina Genovese, R.N.; Sonah Yoo, R.Ph.; Robert Sturwold, R.Ph., and Mr. Willie Ford. This study was supported by the National Institute of Drug Abuse (DA12382-01 to DCD). In addition, the authors acknowledge support from the (1) Department of Veterans Affairs Schizophrenia Biological Research Center (John Krystal), (2) National Institute of Mental Health (MH61019-02 to DCD), (3) National Institute of Alcohol Abuse and Alcoholism (R03 AA11413-02 to DCD), (4) Stanley Medical Research Institute (DCD), and (5) Donaghue Foundation (DCD).
Disclosure/Conflict of interest
None of the authors have any potential conflict/s of interest relating to the subject of the report.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Table S1
Motor results (means [±SD]) (DOC 36.0 KB)
Rights and permissions
About this article
Cite this article
D’Souza, D.C., Braley, G., Blaise, R. et al. Effects of haloperidol on the behavioral, subjective, cognitive, motor, and neuroendocrine effects of Δ-9-tetrahydrocannabinol in humans. Psychopharmacology 198, 587–603 (2008). https://doi.org/10.1007/s00213-007-1042-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-007-1042-2